





Abstract
A 77-year-old male presented with symptomatic, severe aortic stenosis, for which he underwent an aortic valve replacement with the Edwards Inspiris Resilia bioprosthetic valve. After removal of the cross-clamp, a greater than mild transprosthetic cuff leak through a defect between the sewing ring and valve stent post was identified on transesophageal echocardiogram leading to the subsequent need for valve explant and new valve implantation.
Introduction
The Inspiris Resilia Aortic Valve (INSPIRIS; Edwards Lifesciences Corporation, Irvine, CA, USA) is a bioprosthetic aortic valve that is based on the Edwards Magna Ease aortic valve design. It is widely used by surgeons due to its favorable hemodynamics, potential for slower structural deterioration, and superior ability to accommodate future valve-in-valve procedures [1]. Trace and mild transprosthetic cuff leaks have been described previously for the Inspiris Resilia bioprosthetic aortic valve, which have largely been treated conservatively with protamine and separation from bypass [2–5]. Herein, we report a case of an Inspiris Resilia valve implanted into the aortic annulus with a clinically significant transprosthetic leak that required valve explant and new valve implantation.
Case report
A 77-year-old male with a history significant for heart failure with reduced ejection fraction (35%–40%), history of paroxysmal atrial fibrillation status post ablation now in sinus rhythm, hypertension, hyperlipidemia, and diabetes, presented with symptomatic, severe aortic stenosis. Transthoracic echocardiogram demonstrated the aortic valve to be heavily calcified and suspected to be bicuspid, with a mean gradient of 30 mmHg and a calculated valve area of 0.8 cm2. The patient agreed to undergo surgery.
Cardiopulmonary bypass was initiated via central aortic and dual-stage venous cannulation. The aorta was cross-clamped and antegrade del Nido cardioplegia solution was used. A transverse aortotomy was performed, and the aortic valve was noted to be bicuspid and heavily calcified. The aortic tissue at the base of the aortic root was somewhat thinned out with myocardium visible with a characteristic sinking sinus. After the aortic leaflets were excised and annulus debrided, the annulus was sized to a 27 mm Inspiris Resilia valve. The bioprosthetic valve had no obvious defects and it was placed onto the annulus in a supra-annular fashion with multiple ventricularly based 2-0 Ethibond EXCEL (ETHICON, Inc., Somerville, NJ, USA) pledgeted mattress sutures and secured with the COR-KNOT DEVICE (LSI Solutions, Inc., Victor, NY).
After the aortic cross-clamp was removed, transesophageal echocardiogram (TEE) demonstrated what was suspected to be a mild-to-moderate paravalvular leak along the non/right coronary cusp commissure. The jet appeared highly eccentric and perpendicular to the flow of the left ventricular outflow tract (Fig. 1). Given the size of the leak, it was decided to rearrest the heart. After reopening the aortotomy and assessing the bioprosthesis, no valve defects were seen. But given the suspected friable and thin annular tissue, the base of the aorta was further reapproximated and reinforced to the external sewing ring at the right/noncoronary commissure with multiple prolene, pledgeted sutures. After the second cross-clamp was removed, TEE demonstrated a larger, now broad-based, moderate or greater regurgitant leak at the non/right commissure, and, in addition, the presence of a new mild leak along the left/right commissure (Fig. 2). At this point, a transprosthetic leak was suspected with potential malfunction of the valve. The heart was rearrested for a third time, and the bioprosthetic valve was reexamined and annulus probed. The valve was explanted without any annular pathology being evident, and examination of the valve on the back table demonstrated a torn area of cloth along the right/non and left/right commissures of the cuff at the level of the stent posts, suspected to be the site of the leaks (Fig. 3). A new same-sized 27 mm Inspiris Resilia valve was chosen, and the valve was placed on to the annulus in a supra-annular fashion with multiple ventricularly based 2-0 Ethibond EXCEL pledgeted mattress sutures, and secured with the COR-KNOT device.
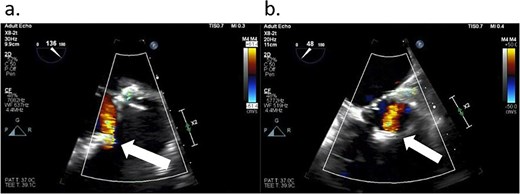
TEE showing a leak (arrows) from the Inspiris Resilia valve in the aortic position after the first aortic cross-clamp was removed. (a) Long axis view. (b) Short axis view.
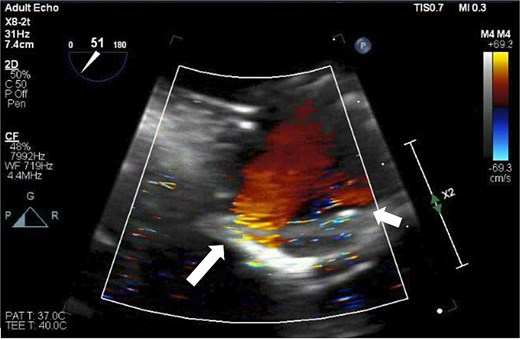
TEE demonstrating two leaks from the Inspiris Resilia valve after the second aortic cross-clamp was removed. A larger now broad-based, moderate or greater regurgitant leak at the non/right commissure (long arrow), and a new mild leak along the left/right commissure (short arrow).
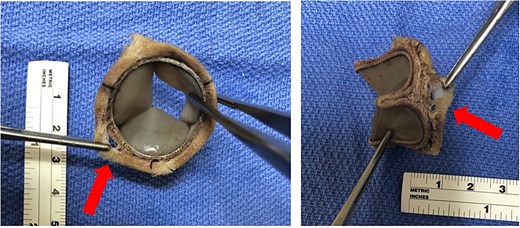
Gross images of the Inspiris Resilia valve showing a small gap (arrows) of the torn fabric between the stent posts and the sewing ring.
After the aortic cross-clamp was removed, TEE did not demonstrate any leaks, and the patient was ultimately weaned from cardiopulmonary bypass. The patient did require placement of a pacemaker for heart block on postoperative day 5, and he was discharged home on day 10 with an otherwise uneventful postoperative stay. The valve was sent back to the valve company, and we have not been informed of any feedback.
Discussion
The Inspiris Resilia valve is well-known to have a transient intravalvular insufficiency attributed to a leak through either the expandable frame of the valve or the valve leaflets [3]. Several sizes of this valve (19 mm through 25 mm) have laser stenciled holes on the wire frame at each of the three stent posts that create a small channel allowing for diastolic flow and can be identified on TEE by their position on the stent post. While both the intravalvular and wireframe hole leaks are known to resolve spontaneously with the administration of protamine or within a short amount of time postoperatively, they can be mistaken for regurgitant jets by the unfamiliar operator and lead to unnecessary intervention [1]. The stenciled holes were not a confounding factor in this case, as a size 27 mm valve was used.
Reports of trace and mild transvalvular leaks typically resolve by being managed conservatively, and one case reported direct suture repair on the cuff [2–5]. In this case, due to the severity of the leak, conservative management with protamine alone was not felt to be adequate. When we rearrested the heart for a second cross-clamp, annular suture reinforcement worsened the leak, which eventually required cross-clamping with valve explant and new valve implantation. The attachment between the cuff and the stent posts provides a natural weakening in the cloth in the design of this valve, as there is more separation between the cuff and the posts. As has been previously postulated, excessive traction on the sutures during valve fixation and sewing too close to the edge of the sewing cuff ring with too many sutures may contribute to tearing of the fabric in that area, which may have worsened the leak in our case [6]. After the second cross-clamp, sutures were only placed on the external sewing ring, so a defect inside the ring would not have been addressed. Plus, with the lower profile and narrow cuff of the valve, more attention needs to be made toward precise suture placement. While trace cuff leaks may be treated conservatively, more significant leaks need to be addressed surgically as there may be a defect with the prosthesis.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}