





Abstract
Pediatric traumatic abdominal wall hernias (TAWHs) are rare injuries that result from both low- and high-energy trauma. TAWHs have a wide presentation, ranging from isolated hernias to cases involving severe associated intraabdominal injury. With a limited number of case reports, correct management and prediction of outcome are difficult. This case report describes a 5-year-and-9-month-old girl who developed a TAWH following a 2-m fall onto a stick. Computed tomography of the abdomen was avoided due to the low-energy mechanism, absence of pain, and lack of physical findings beyond a minor abrasion. Serial sonographic evaluation confirmed bowel herniation without evidence of associated intraabdominal injury. After an observational period of 24 hours without complications, the patient was discharged. Ten days later, an uncomplicated elective open herniotomy was performed. Two-month follow-up revealed no additional contacts to the hospital.
Introduction
Traumatic abdominal wall hernias (TAWHs) are the result of blunt trauma to the abdomen that causes increased intraabdominal pressure, disruption of the fascia, and abdominal wall muscle, with subsequent herniation [1]. Pediatric TAWHs are rare, and literature primarily consists of small populations, limiting knowledge of management and outcomes. In recent literature, most cases have been diagnosed with computed tomography (CT) scans and managed with acute surgery [1, 2]. In this paper, we present a case report of a pediatric TAWH, caused by low-energy trauma, diagnosed with sonography, and managed with elective open herniotomy.
Case presentation
A 5 year-and-9-month-old girl presented as a trauma case after a 2-m fall from a tree. The fall was witnessed by her kindergarten teachers. Shortly after falling, the patient was upright. Upon standing up, a bulge was noticed on the left upper quadrant. According to the patient herself, she had fallen on the buttocks and had landed on a stick. The primary trauma assessment (for which the patient was supine) revealed no positive findings apart from a minor abrasion. The abrasion was ~1 × 0.5 cm in size, superficial, and located where the bulge had been noticed (Fig. 1). There was no surrounding ecchymosis. It was not found painful to palpation. Vitals were within normal range, and the patient appeared otherwise unharmed. A focused assessment with sonography did not reveal anything suspicious. Overall, there was no suspicion of underlying pathology, and it was decided to abstain from trauma-CT. The patient was admitted for secondary assessment and observation overnight at the pediatric ward. Upon secondary assessment, only when standing upright, a bulging protrusion reappeared in relation to the abrasion (Fig. 2). Initial suspicion of TAWH emerged. A Sonographic examination, performed the next day by a specialized radiologist, revealed a 1.5 cm defect in the abdominal wall and a hernia sac of three cm containing bowel (Figs 3 and 4). After an uneventful observation period of 24 hours, the patient was discharged and planned for elective surgery. An open herniotomy was performed ten days later, revealing a fascial and muscular defect of 1 cm containing only fatty tissue at this point (Fig. 5). The defect and skin were closed with absorbable sutures, and the patient was discharged the same day as surgery. Two-month follow-up revealed no additional contacts to the hospital.

Photo upon initial assessment, revealing an abrasion and no apparent surrounding ecchymosis. Herniation not evident in supine position.

Photo of the hernia as seen when standing up, upon secondary assessment.
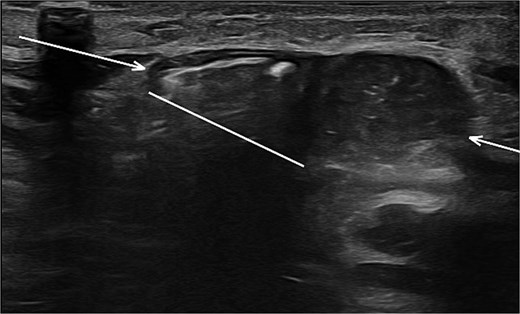
Sonographic imaging of the abdomen revealing a hernia defect (white line) and the hernial sac (white arrows).
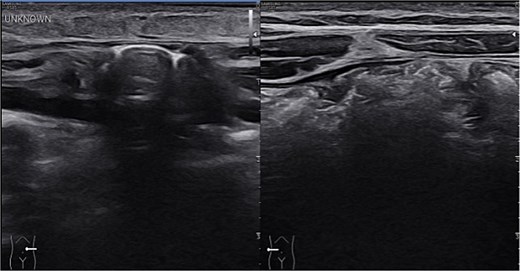
Sonographic imaging comparing left and right upper quadrant. On the left side intestinal content is seen within the hernia sac. On dynamic sonography peristalsis was apparent.

Open herniotomy, revealing a 1 cm defect in fascia and muscular wall, with no evidence of hernia sac or intestinal content.
Discussion
Pediatric TAWHs have been reported both in high-energy trauma and low-energy trauma, commonly from motor vehicle accidents and bicycle handlebar injuries, respectively [2, 3]. This case report, although similar in mechanism to a handlebar injury, presents an upper quadrant TAWH occurring after a low-energy fall, landing on a stick. Reviewing the literature, multiple management strategies have been proposed for TAWHs. The primary concern relates to identifying and managing any underlying intraabdominal injury. Failing to diagnose intraabdominal injury associated with TAWH can have detrimental implications. In terms of approach, it has therefore been debated whether a routine CT scan or even explorative laparoscopy is needed in TAWHs to rule out additional intraabdominal injury [1, 3, 4]. Given the rarity of TAWHs and the small population sizes presented in literature, the risk of associated intraabdominal injury is unknown. In one retrospective cohort study of the 19 confirmed pediatric TAWHs (out of 19.944 pediatric traumas), the frequency of associated bowel injury was 58% [2]. Since the study only included pediatric traumas with abdominopelvic CTs from two level one trauma centers, most cases were high-energy traumas. This limits the generalizability to other cases, like the low-energy TAWH presented in this case, where no CT scan was performed [2]. A systematic review of cases of classic “handlebar” hernias in bicycle accidents reported a 26% risk of underlying intraabdominal injury [5]. With primarily case reports relying on, however, publication bias may skew the prevalence of associated injury. Therefore, estimating the risk of associated injury remains a challenge. With radiation-induced malignancy in mind, especially in children, indiscriminate use of CT scanning in pediatric traumas is a concern. Clinical assessment tools have been developed to aid in appropriate usage of CT-scans in pediatric abdominal blunt trauma. To our knowledge, the incorporation of TAWH as a risk factor in relation to blunt abdominal trauma is yet to be described in such tools [6]. To avoid unnecessary radiation exposure and surgical risk, literature suggests that a differentiated approach, limiting radiation exposure, can be applied when associated intraabdominal injury is found unlikely [4, 6]. To correctly identify such cases, multiple indicators have been associated with a low risk of underlying injury. For TAWHs, low-energy traumas and negative abdominopelvic CT scan, has been the predominant-suggested factors. Additionally, no presence of seatbelt or handlebar sign and no reported pain are factors thought to be associated with low-risk of underlying injury [2, 7, 8]. Ultimately, the clinician management plan relies on a case-by-case evaluation. This case report presents a low-energy pediatric upper quadrant TAWH, where an approach with minimal radiation exposure and an outpatient elective surgical strategy, was found to be appropriate. This case supports a general clinical awareness of the existence of TAWHs in blunt pediatric abdominal trauma and a recognition of the potential severe intraabdominal associated injury. It also highlights that, although high suspicion must remain for underlying pathology, in select cases, a differentiated approach can be applied. In this case, management was based on the low-energy mechanism of injury, negative findings upon physical exam, an uneventful observational period, and repetitive sonography without findings suggestive of associated intrabdominal pathology. An approach with no radiation exposure and minimally invasive surgery was chosen, and the patient was treated successfully.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}