





Abstract
In this case, we present a case of a 48-year-old male patient. The patient initially presented with upper abdominal discomfort, but lacked typical clinical features. As the disease progressed, the upper abdominal pain worsened and was accompanied by symptoms of nausea and vomiting. After admission, the patient received conservative treatment to manage the intestinal obstruction. After 9 days of treatment, the symptoms persisted and worsened, so an open exploratory surgery was performed to clarify the diagnosis and for further treatment. The diagnosis was confirmed intestinal obstruction caused by gastric stones during the operation. The patient recovered smoothly after the operation. This case was easily misdiagnosed as a lesion in the ileal region due to its lack of typical clinical and imaging features, which could have resulted in serious consequences.
Introduction
Gastric calculi are stone masses formed in the stomach due to the ingestion of indigestible or indigestible food [1]. The most common clinical manifestation is plant-derived gastric calculi. Patients can show symptoms such as upper abdominal pain and discomfort, nausea, and gastric stones can occur at any age, including infants and the elderly; with the passage of time, gastric stones can continue to increase and occupy the gastric volume, resulting in a decrease in the patient 's appetite, and active, smooth and solid blocks can be palpable in the upper abdomen [2]. The patient in this case initially showed upper abdominal discomfort, but lacked typical clinical features and various auxiliary tests and examinations were difficult to diagnose. With the development of the disease, upper abdominal pain worsened, accompanied by symptoms of nausea and vomiting. In order to make a clear diagnosis and timely treatment, laparotomy was performed. Complete intestinal obstruction caused by gastric calculi was confirmed during the operation. This case provides a clinical treatment experience of intestinal obstruction caused by gastric stones going down to the intestine. The case also emphasizes the necessity of surgical exploration when the patient has typical clinical manifestations of intestinal obstruction caused by unknown causes.
Case report
The patient, male, 48 years old, rural household registration. The patient was admitted with persistent epigastric pain and discomfort lasting over 5 days. He had a 3-year history of diabetes mellitus, regularly managed with oral metformin, and maintained good glycemic control. He had a history of diabetes for 3 years, regularly took metformin orally, and his blood glucose was well controlled. The patient complained of persistent abdominal pain and discomfort after eating 5 days ago, with abdominal distension and occasional nausea, no vomiting, diarrhea, hematochezia, acid regurgitation, hiccups, belching, chills, and fever. Since the onset of the disease, the patient's spirit, appetite, and sleep were poor, no stool, and normal urination. The weight did not drop. The physical examination showed normal temperature, slightly raised upper abdomen, visible intestinal type, no peristalsis wave, total abdominal tenderness (+), mainly in the upper abdomen, no muscle tension and rebound pain, mobile murmur (−), bowel sound hyperactivity, and the sound of air over water could be heard. Auxiliary examination: abdominal computed tomography (CT) suggested: gallbladder stones, intestinal obstruction, and uneven thickening of intestinal wall (Fig. 1).
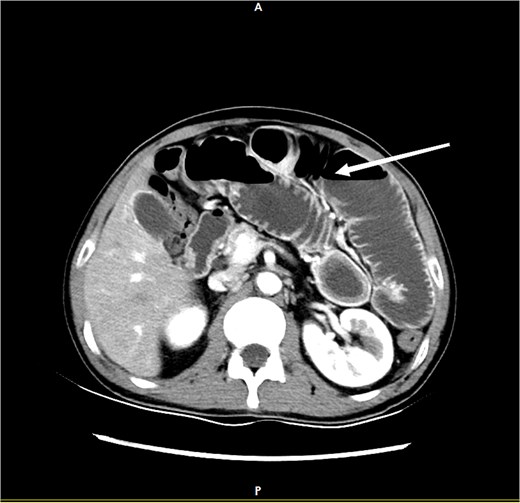
CT demonstrates features of intestinal obstruction as marked by the white arrow.
Diagnosis on admission: (i) Acute intestinal obstruction; (ii) Electrolyte disorders (low sodium, low chloride, and low calcium); (iii) Diabetes mellitus; (iv) Gallbladder stones. After admission, water and fasting were immediately given, gastrointestinal decompression, enema, and maintenance of water and electrolyte balance. Further improvement of gastroscopy and colonoscopy showed no obvious abnormalities, and the patient's symptoms improved after conservative treatment. A total of 8 days after admission, the patient experienced worsening epigastric distension and pain. A gastrointestinal contrast study revealed an obstructive lesion located at the terminal ileum (Fig. 2). On the 9th day after admission, an exploratory laparotomy was performed. During the operation, a mixed-type stone measuring ⁓5×5 cm was found ⁓20 cm from the ileocecal valve. A small intestine incision was made to remove the stone, and the specimen was sent to the pathology laboratory for component analysis. Postoperatively, gastrointestinal decompression was continued, and the patient was kept nil by mouth for 6–8 days. The patient was advised to consume a small amount of warm saline, which was tolerated well without discomfort. Subsequently, the patient was allowed to consume a small amount of liquid diet, which was also tolerated without issues. Gastrointestinal decompression and fasting were then discontinued. On the 10th postoperative day, the patient had a bowel movement, indicating that the obstruction had been resolved, and no stenosis was observed at the ileal anastomosis site. The pathology laboratory reported that the submitted specimen consisted of a mixture of cellulose, hemicellulose, and tannic acid. Inquiry of medical history: the patient had previously had discomfort such as upper abdominal distension and pain, occasional nausea and loss of appetite, etc., which were not paid attention to and treated. According to the postoperative pathological component detection combined with clinical manifestations and the patient 's medical history, it can be considered that the terminal ileum stones are derived from gastric stones (Figs 3 and 4).
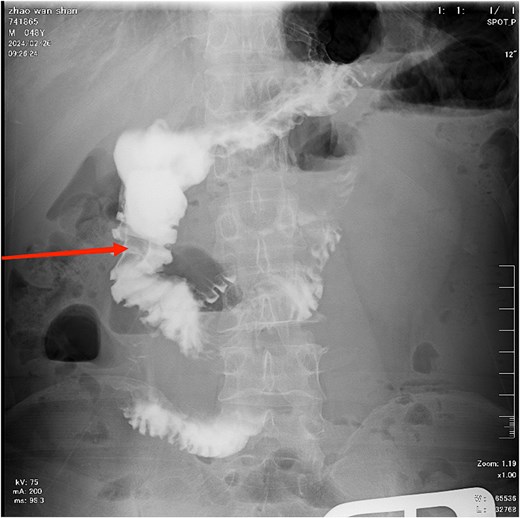
The contrast study reveals a complete obstruction at the terminal ileum, as indicated by the arrow.
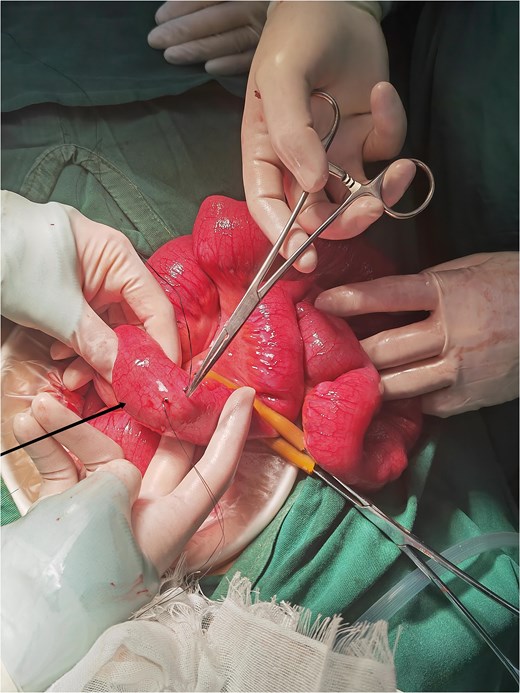
Localization of the calculus during surgery.

The black arrow indicates the gastric bezoar, and the white arrow marks the site of stone extraction.
Discussion
Gastric calculi is a rare disease, and the common pathogenic factors include previous history of chronic gastric disease [2], hypothyroidism and other abnormal gastric peristalsis. It is common in plateau areas of China, especially the oval mixed type gastric calculi [3]. These calculi are usually produced by tannic acid in persimmon, hawthorn and other foods after the reaction with gastric acid, and deposited in the stomach [4]. For patients with such conditions, if the calculi pass through the pylorus into the small intestine but become embedded in the terminal ileum, it may cause intestinal obstruction [5]. Although drug dissolution and endoscopic removal are one of the treatment methods, the effect is not ideal for large calculi that cause intestinal obstruction, and laparotomy is needed. In addition, in terms of classification, gastric calculi can be divided into botanical, animal, drug and mixed. Among them [6], botanical is the most common, and due to the lack of calcium salts, it is difficult to show typical or obvious calculi on imaging. This paper introduces a case of a middle-aged male patient [7]. The patient did not eat foods that are easy to cause gastric calculi, but had corresponding manifestations, and was finally diagnosed as complete intestinal obstruction [8]. It is worth noting that in this case, due to the lack of typical clinical manifestations and imaging features, it is easy to be misdiagnosed as other problems and delay the opportunity for cure. Therefore, when a patient has a history of digestive problems and a history of eating certain foods that can cause gallstones and suddenly develops related symptoms [9], the doctor should be highly suspicious of a similar condition and take appropriate measures to avoid more serious consequences [10].
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}