





Abstract
Angiolipomas are relatively rare in the head and neck, are usually ˂4 cm in diameter, and may recur if not completely excised. We aim to describe a clinical case of a healthy 25-year-old man who presented with a large mass extending from the root of the neck to the skull base, adjacent to the major vessels, as demonstrated by a magnetic resonance imaging scan. The mass was excised under general anesthesia, with Careful avoidance of injury to the major vessels, which posed a challenge during the surgery. Pathology confirmed the diagnosis of angiolipoma. One year of follow-up showed no recurrence. In conclusion, angiolipoma can present as a giant cervical mass in close relation to the carotid sheath, requiring careful excision to avoid both injury and recurrence.
Introduction
Neck masses are common in adults and can arise due to various etiologies [1]. They can be classified into infectious, inflammatory, congenital, traumatic, benign, or malignant neoplastic masses [1]. Among benign neoplastic masses, lipomas are relatively rare and account for 1% of neck masses [2]. Lipomas are subclassified into several subtypes, including simple lipoma, fibrolipoma, mixolipoma, chondroid lipoma, angiolipoma, angio-myolipoma, myelolipoma, spindle cell lipoma, sialolipoma, pleomorphic lipoma, and atypical lipoma [2]. We aim to report a case of a cervical angiolipoma, which was unusually large and posed a challenge during surgery due to its proximity to the main vessels and its broad extent.
Case presentation
A healthy 25-year-old man with a large lateral right neck mass was referred to us. He had cosmetic concerns without any other symptoms. The mass first appeared several years ago as a small, nontender swelling in the right lateral neck. Over the years, the mass gradually increased in size and became a cosmetic issue. The patient had a history of a neck mass at the same site with a similar clinical course 12 years ago. That mass was excised without histopathological examination; however, the similar clinical course raises the possibility of the current mass being recurrent. The patient reported no use of tobacco, alcohol, or illicit drugs and had no significant family history.
The physical examination revealed a nontender, well-defined, mobile, firm mass measuring ⁓15 cm in the right lateral neck, extending from the sternal notch superiorly to the mandibular angle. The mass showed no skin changes or fixation to the skin. Examination of the cranial nerves was normal, there was no clinical lymphadenopathy, and the oral examination showed no abnormalities.
A neck ultrasound revealed a well-defined, solid, mildly hyper-echoic, heterogeneous subcutaneous mass located on the right side of the neck. A contrast-enhanced MRI scan showed a 14 cm diameter, well-demarcated, high-signal, non-homogeneous mass adjacent to the carotid artery and thyroid gland (Figs 1 and 2). The radiologist suggested lipoma as the most probable diagnosis. Ultrasound-guided fine-needle aspiration (FNA) of the mass identified some lipocytes and fibrocytes but no malignant cells.

T2-weighted MRI image showing the relationship between the mass and the carotid sheath (indicated by the arrow).
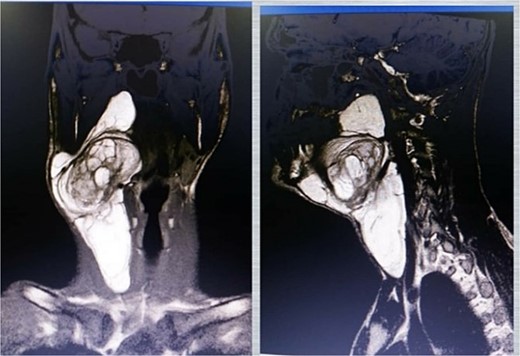
MRI images showing a high-signal mass on both T1 (left) and T2 (right) sequences.
One month after the referral, an excisional surgery was performed. The procedure began with a skin incision through the platysma muscle, followed by dissection beneath the superficial layer of deep cervical fascia (SLDCF) to identify the mass (Fig. 3). Next, we identified the carotid artery after dissecting the inferior pole of the mass from it and proceeded superiorly with great caution (Fig. 4). The mass was completely removed without disturbing its capsule. The mass was observed grossly as an encapsulated, reddish, lobulated mass (Fig. 5). Due to the extensive dissection and the large size of the mass, a drain was placed and then it was removed 2 days after. The patient was subsequently discharged home without any noticed complications. The pathology results were consistent with angiolipoma (Figs 6 and 7). A 1-year follow-up revealed no recurrence.

Operative image showing the mass after flap elevation.
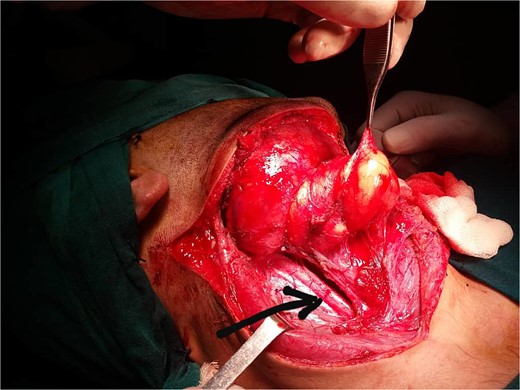
Operative image showing the relationship of the mass to the carotid artery (black arrow).

Gross image of the excised lesion, appearing as a reddish, lobulated mass.
![Microscopic view of the lesion showing a large fatty component with scattered islands of capillary vessels. These findings suggest angiolipoma [6].](https://oupdevcdn.silverchair-staging.com/oup/backfile/Content_public/Journal/jscr/2025/2/10.1093_jscr_rjaf079/1/m_rjaf079f6.jpeg?Expires=1788190042&Signature=BPfYPzqd76UBSMcqsNwR46I66yv~ixIsVRQynB0G728CVhaNk1JDUqXr9g77kcn93I~JwLRRqkW-lecqi84rs5ryf-dApt219WGn14vDogW6wVq8CxAVePbBu3Dz6M9OaqTsjVShyg4dVLcMdR-xEOMTSdftM2NchmuYa4-KCxDMPiuNmsnCTm0TvI5Da7XhAtjqqG9tDF6B2Jg~IcUdefSo7JT9Bev~kAAaCDloZc0mneTwuvA3plMnNSsgtWAaG4emQSjaZSR4iqJKfsh0ziYnTrtVnTTL3-Qlf0z41zOPjSiRXsxoQYMelrkxHG1DrrG16c1jMaNxPlqh3BJfxg__&Key-Pair-Id=APKAIYYTVHKX7JZB5EAA)
Microscopic view of the lesion showing a large fatty component with scattered islands of capillary vessels. These findings suggest angiolipoma [6].
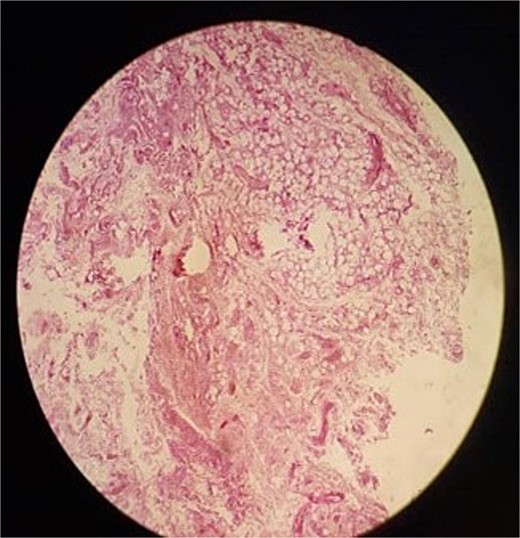
Another microscopic view of the lesion.
Discussion
Angiolipoma is a subtype of lipoma consisting of two components: fatty and vascular, with varying degrees of contribution from each [3]. It comprises 5%–17% of all lipoma cases (lipoma accounts for 1% of neck masses), as shown in two relatively old studies [4, 5]. There are no current statistics on the overall incidence of angiolipoma.
Most angiolipomas are sporadic with no known causes. However, some potential risk factors have been reported in the literature, including familial deposition (familial angiolipomatosis) [6] and certain drugs (indinavir, long-term steroids) [7, 8]. Previous case reports showed that angiolipoma may present anywhere in the head and neck, including intracranial, spinal, and visceral locations. Subcutaneous angiolipomas usually present as tender, slowly growing masses with rare skin discolorations and possible compressive symptoms [9]. They are usually ˂4 cm and more common in adolescents and young adults [10]. Our patient had cosmetic issues without other complaints.
Any neck mass should be evaluated according to AAO-HNS guidelines for neck masses in adults, using physical examination, imaging modalities, and/or FNA biopsy to assess it for malignancy [1]. A study found that most angiolipomas are hyperechoic on ultrasound, and usually, the blood flow within them cannot be determined with color Doppler [11]. Another study showed that angiolipoma has a variable appearance on MRI scan (fat nodules with or without low signal-intensity areas of various sizes and locations that correspond to capillary areas), suggesting that it’s not entirely possible to differentiate it from lipoma [12]. Therefore, the definitive diagnosis is made by pathology. In our case, the findings led us to consider lipoma as the most probable diagnosis and reasonably, though not definitively, exclude malignancy.
Angiolipoma has two distinct types: noninfiltrating and infiltrating, with different pathological features and prognoses. Noninfiltrating angiolipomas are more common and encapsulated, whereas infiltrating lesions lack a capsule and may recur if not completely excised with clear margins. Complete surgical excision of the former is curative, with a very low rate of recurrence, while infiltrating lesions tend to recur in up to 50% of cases [10]. In our case, the lesion was encapsulated, with no recurrence at 1 year.
Angiolipoma has no risk of malignant transformation [10]. It may present in the neck as a small, asymptomatic mass. However, the recommended treatment for such a lesion, as with all angiolipomas of the neck, is total surgical excision because it does not regress spontaneously and may enlarge, becoming symptomatic or a cosmetic issue [9, 10].
In this case report, the angiolipoma was unusually large, adjacent to the carotid artery, and required careful planning and meticulous dissection to ensure complete excision and prevent recurrence, while avoiding injury to the major vessels by identifying them at the start of the surgery.
Conclusion
Angiolipoma of the neck can present as a giant mass in close proximity to important structures requiring careful, complete resection to avoid both injury and recurrence.
Author contributions
Dr. Alaa Ahmad was the main surgeon, supervised the patient's case, and refined the manuscript. Dr. Mounir Barakat served as an assistant surgeon, collected patient data, and revised the manuscript. Dr. Yousef Salameh was a surgeon's assistant, wrote the case presentation, and revised the manuscript. Dr. Amjad Al-ali reviewed the literature on relevant topics, wrote the discussion section, and revised the manuscript.
Conflict of interest statement
None declared.
Funding
None declared.
Informed consent
A signed informed consent was obtained from the patient to publish this case presentation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}