





Abstract
Epulis fissuratum (EF) is a benign fibrous hyperplasia of the oral mucosa caused by chronic trauma, usually linked to prolonged use of poorly fitting prostheses. This condition compromises phonation, chewing, and aesthetics, thus affecting quality of life. We report the case of a patient who had worn complete upper dentures for three decades and developed EF. Management required two stages. First, the lesion was excised with a scalpel, obtaining tissue for histopathological confirmation. Three months later, a second surgery was performed with a free gingival graft to deepen the vestibule and create an adequate keratinized gingival band. At three months, follow-up showed proper healing, favourable soft tissue recovery, and no recurrence, enabling future rehabilitation. This case illustrates that sequential management, combining surgical excision and gingival grafting, provides a predictable and reliable alternative for advanced EF, ensuring functional recovery and improved prognosis.
Introduction
Epulis fissuratum (EF) is considered a non-malignant reactive entity characterized by fibrous hyperplasia of the oral mucosa, usually caused by chronic trauma [1–3]. It has a predilection for elderly patients, with a certain inclination towards females and a more prevalent location in the mandibular vestibule [1, 2]. Despite being considered a benign entity, it has been shown that the persistence of an irritative stimulus promotes both recurrence and, in unusual cases, may be linked to malignant transformation [1, 3].
Although several modalities have been documented in the literature, there is no consensus or standardized protocol for the treatment of EF, which highlights the importance of individualizing management based on the clinical particularities of each case and the available resources [4–7]. The objective of this manuscript is to describe a clinical case of EP in a patient with a removable total dental prosthesis, emphasizing the surgical approach through excision of the entity, removal of excess tissue, and placement of a free gingival graft as a comprehensive strategy to restore function, oral health, and prevent recurrence.
Case presentation
A 70-year-old male patient with no pathological history, who had been wearing a full upper denture for 30 years without ever removing it, presented at the dental clinic. Intraoral examination revealed a firm, fibrous, smooth mucogingival tissue growth measuring ~ 5 × 4 cm with no signs of active ulceration. Its base originated from the bottom of the vestibule, being a pedunculated base and extending to the residual alveolar ridge, adopting a morphology of multiple folds, which corresponds to the friction of the overextended edge of the prosthesis (Fig. 1a and b). The patient reported difficulty chewing and speaking but did not report pain or a history of trauma or surgery in the area.
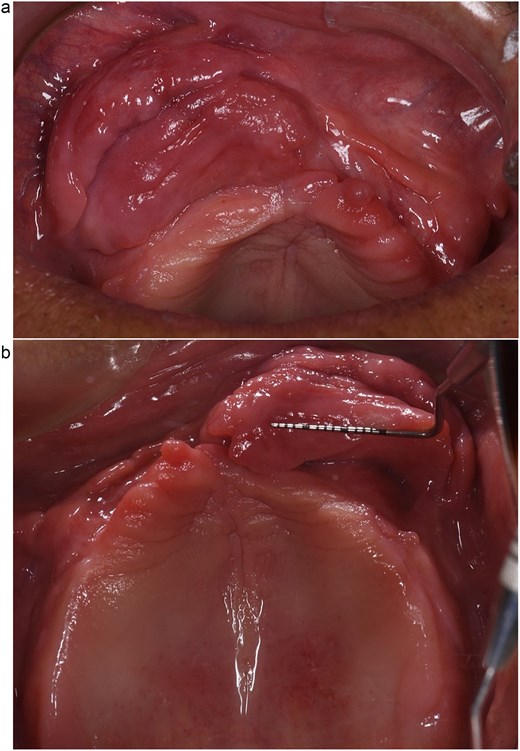
Clinical image of multiple folds with a firm, fibrous, smooth appearance and no signs of active ulceration. (a) Front view. (b) Occlusal view.
The first surgical procedure consisted of applying local anesthesia with 4% articaine with epinephrine 1:100 000 under aseptic and antiseptic conditions. Next, using a 15c scalpel blade, the hyperplastic fibrous folds found in the upper vestibule were removed, considering the appropriate margins to ensure complete resection of the pathological tissue. The removed tissue was placed in 10% formalin for subsequent histopathological analysis. To promote edge approximation and achieve primary healing, the surgical wound was sutured with 4–0 Vicryl using simple stitches (Fig. 2). An antibiotic regimen (amoxicillin 500 mg every 8 hours for 7 days) and an analgesic regimen (ibuprofen 600 mg every 8 hours for pain) were prescribed, in addition to rinsing with 0.12% chlorhexidine for 10 days. Postoperative follow-up consisted of check-ups at 7 and 15 days, the latter of which involved the removal of the sutures without complications. Histopathological analysis revealed an EF (Figs 3, 4a and b).
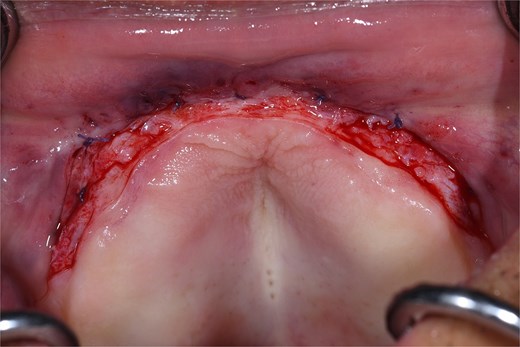
Intraoperative view of the anterior vestibular area during the first surgical procedure, after complete removal of the epulis fissuratum. The surgical bed is identified with defined margins, correct control of hemostasis, and preservation of adjacent healthy tissue.
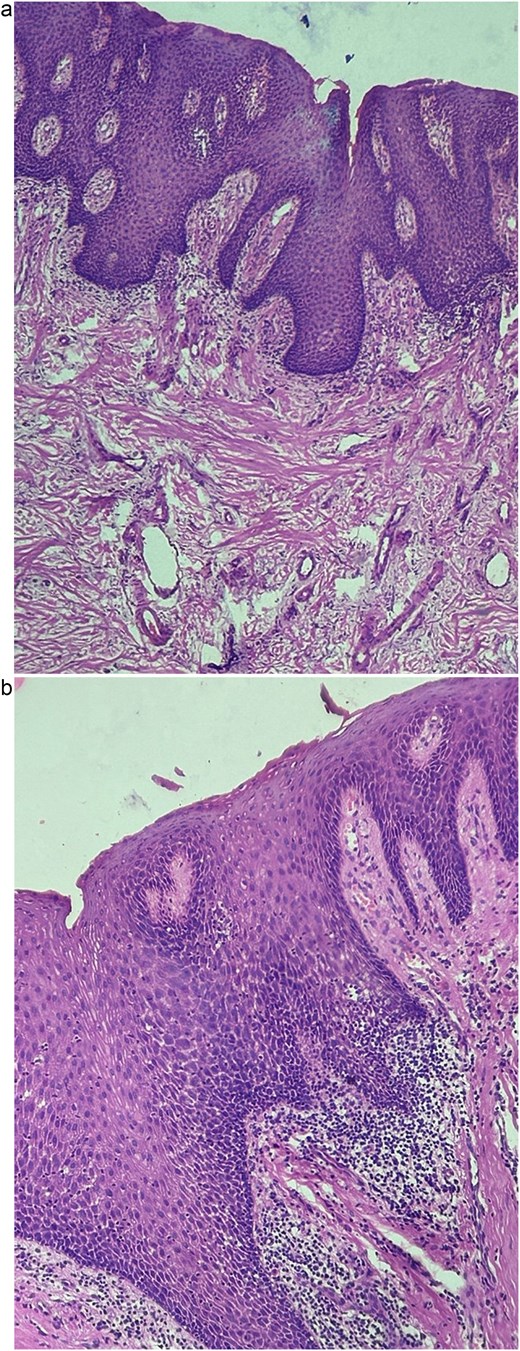
(a, b) Mucosa with acanthosis of the non-keratinizing stratified squamous epithelium with mixed inflammatory infiltrate.
The second surgical procedure consisted of designing a recipient bed through a partial flap in the anterior vestibular area under infiltrative anesthesia with 4% articaine. Next, a free gingival graft measuring ~48 × 5 mm was obtained from the palatal area, which was presented, adapted, and stabilized to the recipient bed with 6–0 nylon sutures, using the technique of simple interrupted stitches and sutures to the periosteum (Figs 5 and 6). Postoperative follow-up consisted of check-ups at 7, 15, and 20 days, with the sutures being removed without incident at the 20-day check-up.
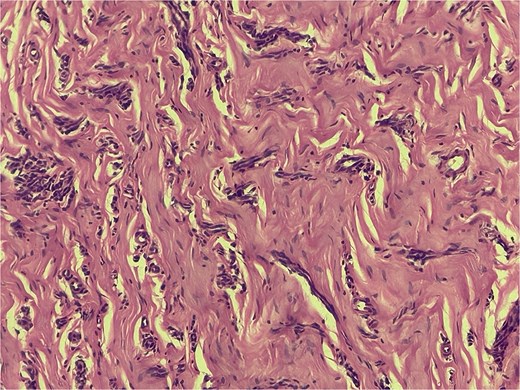
Hypertrophy of collagen fibers on the lamina propria, with intertwining between them. Blood capillaries are observed to be collapsed with scattered chronic inflammatory infiltrate.

Free gingival graft measuring ~48 × 5 mm taken from the palatal area, presented on a sterile wooden board for handling, prior to adaptation and stabilization in the recipient site.
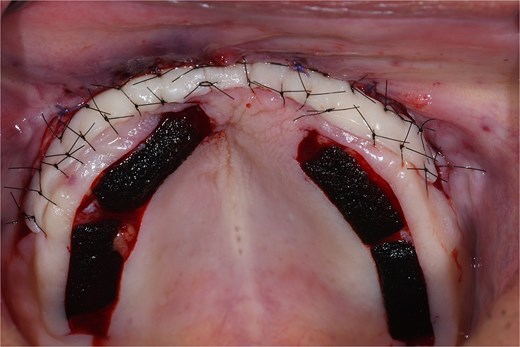
Free gingival graft placed in the anterior vestibular area and stabilized with 6–0 nylon, using the interrupted single stitch technique. The donor site was protected with a collagen sponge to promote hemostasis.
After a 3-month follow-up period, adequate healing and proper soft tissue recovery were observed. There was no evidence of inflammation, infection, or related complications (Fig. 7).
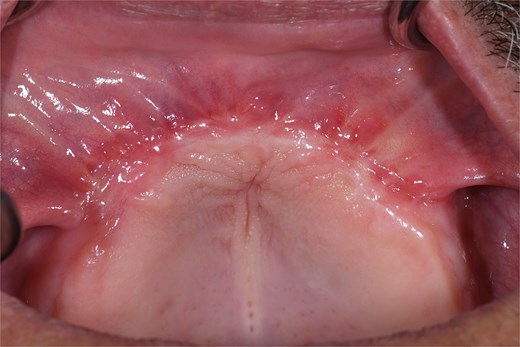
Clinical evolution three months after the second procedure, showing adequate healing, total integration of the gingival graft, and development of a stable keratinized gingival band.
Discussion
Conventional scalpel surgery is the first line of treatment for EF, and depending on clinical conditions, additional techniques should be considered as a complement. This case highlights the importance of comprehensive surgical management in two phases, which are consistent with previous studies [8]. First, surgical removal of the entity allowed for the removal of hyperplastic fibrous tissue and confirmation of the diagnosis through histopathological study, which is essential for ruling out more biologically aggressive lesions. Second, the insertion of free gingival graft not only allowed for the creation of vestibular depth but also formed an adequate band of keratinized gingiva. This feature is especially important, as a considerably wide keratinized tissue provides better resistance to prosthetic friction, contributes to the maintenance of dental plaque control, and minimizes the occurrence of long-term recurrence. This therapeutic approach contrasts with that of Khalifa et al. [1], who demonstrated the success of a single procedure that integrates EF removal with vestibuloplasty and gingival grafting in a single surgical session. In this sense, the strategy implemented confirms that the choice between single or staged surgical intervention should be customized according to the extent of the lesion, clinical particularities, and future prosthetic objectives.
On the other hand, surgical treatment modalities based on energy technologies such as diode laser, CO₂ laser, or cryosurgery are highly effective in the management of small or moderate-sized lesions but have limitations when considered for large fibrous hyperplasias [6, 9, 10]. These methods offer significant advantages, including immediate hemostasis, reduced postoperative pain and inflammation, and accelerated healing compared to conventional techniques [5, 6, 11]. In this scenario, surgical intervention with a conventional scalpel remains the first-line treatment option for large lesions, as it allows for more accurate and reliable surgical control, enables the delimitation of adequate margins, and, most importantly, guarantees the collection of intact tissue for histopathological analysis [1, 6, 8].
The success of EF management does not depend exclusively on the surgical intervention implemented, but also on the patient’s adherence to postoperative instructions and the elimination of causal factors. Consequently, the manufacture of a new prosthesis with the appropriate design, instructions on oral hygiene measures, and the recommendation not to use the prosthesis at night are essential strategies for preventing recurrence.
Conclusion
This clinical case demonstrates that surgical treatment involving two procedures is an effective alternative for managing large EF in patients with full dentures. This approach highlights the importance of personalizing treatment according to the size of the lesion, functional requirements, and the patient’s rehabilitation goals.
Author contributions
Sarah Monserrat Martínez-Lomelí: (Formal analysis, Investigation, Conceptualization, Writing—review & editing), Luis Antonio Gonzalez-Gomez (Validation, Writing—review & editing), Eder Javier Martínez-González (Methodology, Validation, Writing—review & editing), Mario Alberto Alarcón-Sánchez (Conceptualization, Validation, Methodology, Writing—review & editing), Francisco Javier Alcaraz-Baturoni (Investigation, Conceptualization), Miguel Angel Robles-García (Writing—review & editing), Vini Mehta (Conceptualization, Writing—original draft, Writing—review & editing) and Artak Heboyan (Supervision, Conceptualization, Writing—original draft, Writing—review & editing)
Conflict of interest statement
All authors report no relevant conflicts of interest for this article.
Funding
None declared.
Data availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Patient informed consent
The study participant provided informed written consent prior to study enrollment.
CARE Checklist (2016) statement
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}