





Abstract
A thoracic kidney is a scarce type of ectopic kidney. We report the case of a 76-year-old man who developed cancer of the ureter, ipsilateral to the thoracic kidney. He presented with abdominal pain in the right upper quadrant. Computed tomography revealed a right hydronephrotic kidney located in the thorax with elevation of the diaphragm. Further examination uncovered a cT2N0M0 ureteral cancer in the right upper ureter. A laparoscopic radical right nephroureterectomy was performed using a retroperitoneal approach. The retroperitoneal space was created for the usual port placement. A port between the 11th and 12th ribs was added to facilitate handling the suprahilar area, specifically the dissection of the superior aspect and separation of the kidney without accompanying pneumothorax. To our knowledge, this is the first report of a successful complete laparoscopic surgery via the retroperitoneal approach for a malignant disease associated with a thoracic kidney.
Introduction
A thoracic kidney is an extremely rare positional anomaly [1]. It is defined as the presence of a kidney in the posterior mediastinum above the level of the diaphragm. It can be asymptomatic and incidentally found unless associated with insufficient childhood lung development [2]. In this report, we describe a case of successful laparoscopic radical surgery for a thoracic kidney with ureteral cancer in the ipsilateral ureter.
Case report
A 76-year-old man visited our hospital with a chief complaint of right upper quadrant abdominal pain. He had undergone low antegrade resection for rectal cancer and resection of liver metastases two decades previously. Computed tomography (CT) revealed pelvic dilatation with minor urinary extravasation in the tissue surrounding the right kidney, which was located in the thorax, with elevation of the diaphragm. He underwent retrograde pyelography, which showed a 3 cm filling defect in the upper ureter, suggesting ureteral cancer. A ureteral stent was placed simultaneously to relieve the symptoms. Urine cytology was positive for urothelial carcinoma, cystoscopy revealed no tumor in the bladder, and CT showed no signs of lymph node or distant metastasis. Ureteral carcinoma was diagnosed as cT2N0M0 (Fig. 1a). In addition, the affected ureter was associated with a thoracic kidney. The origin of the right renal artery and the entry of the renal vein were at the same level as those of the contralateral kidney (Fig. 1b). Shortly thereafter, the patient was referred to our department for surgery. Because the patient had a history of abdominal surgery, a retroperitoneal approach to radical nephroureterectomy was preferred. Renal vascular control was performed via the usual port placement. However, handling the suprahilar area and the superior aspect of the kidney was determined to be challenging due to cephalad deviation. Therefore, an additional intercostal trocar was planned after securing sufficient retroperitoneal space. In cases of insufficient retroperitoneal space for the trocar, a transthoracic approach via thoracoscopic surgery was prepared in collaboration with thoracic surgeons.
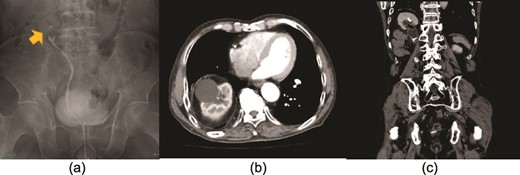
The yellow arrow in the retrograde pyelography shows a ureteral tumor in the upper ureter (a). There were no findings suggestive of metastases, and the clinical diagnosis was right ureteral carcinoma T2N0M0. An axial (b) and coronal (c) computed tomography view show the right kidney in the thorax with protrusion of the diaphragm, suggesting a thoracic kidney.
The patient was placed in the left lateral decubitus position. The retroperitoneal space was created using a PDB balloon dissector (Covidien Ltd., Mansfield, MA, USA). The ports were placed as shown in Fig. 2a. Although the renal vessels could be exposed, vascular control is difficult. Forceps could not reach the suprahilar area via the lateral port because the iliac crest interfered with forceps movement (Fig. 2b). Therefore, according to the preoperative plan, a 5 mm port was added at the intercostal site, as indicated in Fig. 3a. The trocar accessed the retroperitoneal space directly without injuring the pleura or diaphragm. The additional port secured the manual placement of the suprahilar area and ensured safe vascular control. The port also secured the handling of the superior aspect of the kidney and the successful completion of laparoscopic surgery (Fig. 3b). The lower ureter and bladder cuff were dissected, and en bloc specimens were retrieved via a Gibson incision.
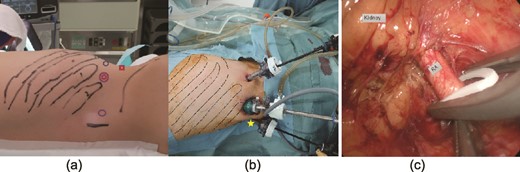
Port position at the beginning of retroperitoneal laparoscopic surgery (a).  indicates the port for the camera, ◯ refers to the 12 mm left and right ports for manipulation, and □ is the 5 mm port site for the assistant. (b, c) Manipulation of renal vessels was complex because the forceps could not reach the suprahilar area through the lateral ports (☆). Dotted lines indicate the ribs. RA: renal artery.
indicates the port for the camera, ◯ refers to the 12 mm left and right ports for manipulation, and □ is the 5 mm port site for the assistant. (b, c) Manipulation of renal vessels was complex because the forceps could not reach the suprahilar area through the lateral ports (☆). Dotted lines indicate the ribs. RA: renal artery.
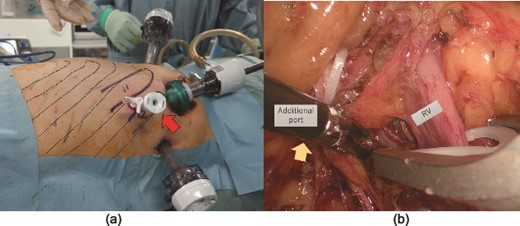
(a) A 5 mm port added at the intercostal site (arrow). Dotted lines indicate the ribs. (b) The additional intercostal port secured access to the supra hilar area (arrow), allowing for safe renal vascular control and manipulation of the superior aspect of the kidney. RV: renal vein.
The total operative time was 6 hr 46 min, including 4 hr 35 min of laparoscopic surgery. The pathological diagnosis was pT2, INFb, Ly0, v0, and RM0 high-grade invasive ureteral carcinoma. The patient’s postoperative course was generally uneventful; however, delirium management was required. The patient was discharged from the hospital on postoperative day seven.
Discussion
Thoracic kidney is a rare form of ectopic kidney. While the exact frequency is unknown, autopsy cases suggest that the prevalence is 3 in 51 880 [1]. A thoracic kidney is congenital, although trauma occasionally causes a similar condition, referred to as an acquired thoracic kidney. Diaphragmatic hernia is also associated with protrusion of abdominal organs. However, the disease is caused by the absence of a muscular layer, and its concept differs from that of a thoracic kidney. It is most often detected incidentally and does not require treatment. Abnormalities in renal elevation have also been reported during fetal life. Notably, during development, both kidneys are located in the lower pelvis; however, at 7 to 8 weeks of gestation, they rise with rotation due to caudal growth of the fetal spine and settle into their normal positions, while the diaphragm closes at ~8 weeks of gestation [3]. It has been suggested that a thoracic kidney may develop when the kidney ascends excessively cranially before complete fusion of the posterior aspect of the diaphragm, causing the kidney to be surrounded by the posterior medial aspect of the thoracic canal and the lumbar rib triangular pyramid. The diaphragm then thinly and closely encircles the renal projection [4]. There is a high risk of concurrent urinary tract malformations, such as duplication of the renal pelvis and ureter; however, no findings suggestive of such urinary tract complications were observed in this case report.
Case reports on thoracic kidney surgery have been limited. One previous study reported open transthoracic surgery for children with concomitant developmental lung defects [2]. Another prior study described percutaneous nephrolithotripsy for renal calculi in adult patients [5]. To the best of our knowledge, there are no reports of surgical treatment for malignant diseases of the ipsilateral urinary tract as in the present case. Here, we present the first report of a thoracic kidney successfully resected laparoscopically using the retroperitoneal approach. In this case, we were able to develop a relevant strategy according to the anatomy. This case suggests that a retroperitoneal approach to laparoscopic surgery for a thoracic kidney is safe, although careful considerations and preparations are required.
We describe a case of successful laparoscopic radical surgery for a thoracic kidney in which ureteral cancer developed in the ipsilateral ureter; however, careful considerations and preparations are needed.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the publication of this article.

{kind=link}
{kind=link}
{kind=link}