





Abstract
Since the first use of a da Vinci system to perform a radical tonsillectomy in 2007, transoral robotic surgery (TORS) has been further developed and finally accepted as a safe surgical method. The recent introduction of the da Vinci Single-Port (SP) system has brought new innovations in the field of ears, nose and throat (ENT) medicine, e.g. to perform minimally invasive head and neck tumor surgery. In Europe, the da Vinci SP system has recently received CE Mark approval for TORS application. We present the first case of a robot-assisted bilateral benign tonsillectomy with the da Vinci SP system in Germany and demonstrate the technical feasibility of this platform.
Introduction
The da Vinci system (Intuitive Surgical Inc., Sunnyvale, CA, USA) was introduced in 1999 and approved for human use by the US Food and Drug Administration (FDA) in 2000 [1]. Through continuous development and implementation in various surgical fields over the past 25 years, the da Vinci system is considered the most established surgical robot [2]. The da Vinci Single-Port (SP) system is a specialized version of the da Vinci system designed for minimally invasive single-port surgery. It features a single robotic arm through which an articulating endoscope and up to three articulating instruments are inserted through a single incision or body opening. The da Vinci SP system was initially approved by the FDA in 2018 and received CE Mark approval for use in Europe in January 2024, including for transoral robotic surgery (TORS) [3]. Weinstein et al. [4] reported in 2009 on the use of the da Vinci system for TORS. This report examined the capabilities, safety and efficacy, learning process, functional outcomes, oncologic outcomes, and costs of using the robot for TORS. The use of the da Vinci SP system for TORS has recently been compared with that of previous models, offering advantages in the form of shorter docking times, reduced console times and improved maneuverability and field visualization [5]. However, the experience with the da Vinci SP system for TORS is limited and its usage for TORS has not been described in the European landscape. In this study, we present a recently completed robot-assisted bilateral benign tonsillectomy using the da Vinci SP system. To the best of our knowledge, this is the first application of the da Vinci SP system for TORS in Germany.
Case report
Case presentation
A 36-year-old man presented to our outpatient department complaining of recurrent tonsillitis. More precisely, the patient had five to six episodes of tonsillitis per year, each of which required antibiotic treatment. He had a medical history of psoriatic arthritis, which was aggravated by each episode of tonsillitis. The ears, nose and throat (ENT) examination revealed hyperplastic tonsils with deep crypts but without signs of an acute inflammation. The indication for bilateral tonsillectomy was given.
Operative technique
The robot-assisted bilateral benign tonsillectomy was performed under general anesthesia. The operating table was set to the lowest position. The patient was placed in supine position and the patient’s head was carefully reclined. We used the da Vinci SP system to perform the procedure. This robotic surgical system consisted of the following parts: the surgeon console, the vision cart, and the patient-side cart. The configuration of the operative room for the procedure is shown in Fig. 1.
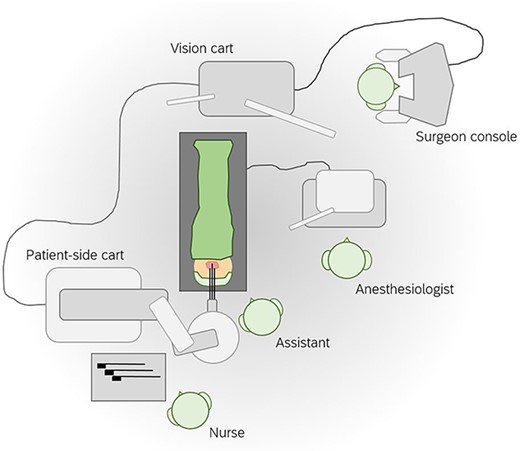
Configuration of the operative room for robot-assisted bilateral benign tonsillectomy using the da Vinci SP system. The da Vinci SP system is a robotic surgical system in three parts: the surgeon console, the vision cart, and the patient-side cart.
We opted for transnasal intubation to avoid oral and oropharyngeal obstruction by an orotracheal tube. A McIvor blade was used for the exposure of the tonsil region. Subsequently, the patient-side cart was positioned on the left side of the patient and the robotic arm of the patient-side cart was aligned so that the single-port cannula was 10 cm above the opened mouth. Then, the articulating endoscope and two articulating instruments were inserted: one monopolar cautery instrument, one Maryland bipolar forceps. All instruments pointed to the tonsil region. We set the custom remote center (a fixed point in space around which the robotic arms move) ~2 cm in front of the maxillary teeth. The configuration of the patient-side cart and the position of the robotic arms are shown in Fig. 2. The assistant was placed on the patient’s head to enable active surgical assistance using suction (suction of blood and smoke) and the angled side of a raspatorium (exposure of the tissue and creation of tissue tension during the surgeon’s dissection).
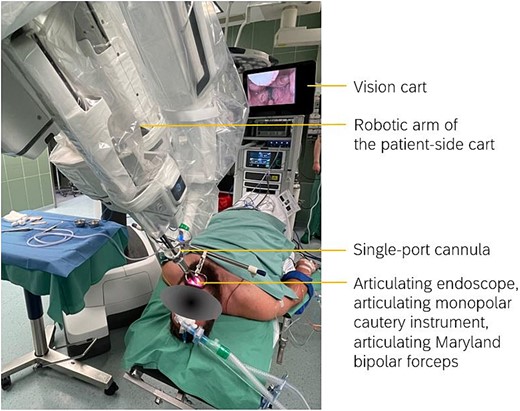
Configuration of the patient-side cart and the position of the robotic arm. The single-port cannula was aligned 10 cm above the opened mouth. One articulating endoscope and two articulating instruments were inserted into the single-port cannula: one monopolar cautery instrument, one Maryland bipolar forceps. The custom remote center was set approximately 2 cm in front of the maxillary teeth.
The surgical procedure was performed starting on the right side. The endoscope was aligned so that the right tonsil was displayed in the central field of view. The medial face of the right tonsil was then further medialized with the Maryland bipolar forceps. The raspatorium was hooked onto the right palatoglossal arch to create tension. Then, the mucosal incision was made in the area of the upper tonsil pole with the monopolar cautery instrument until the tonsil capsule was reached. Subsequently, the tonsil was dissected along the capsule to the lower pole and finally removed. Bleeding was stopped intermittently with the Maryland bipolar forceps while the monopolar cautery instrument and the assistant’s raspatorium were used to push away any collapsing tissue. Before moving to the left side, all instruments were retracted and cleaned. The positions of the Maryland bipolar forceps and the monopolar cautery instrument were switched. We used the monopolar cautery instrument for the surgical dissection; therefore, it was installed on the lateral side of the single-port facing the surgical dissection. All relevant surgical steps are shown in Fig. 3. The docking time was 8 minutes, the operation time 37 minutes. No significant intraoperative events were observed.
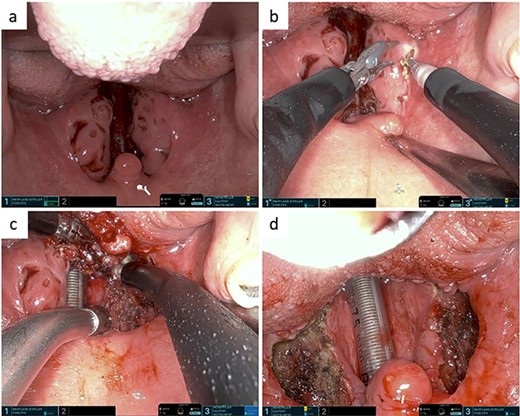
(a) Pre-tonsillectomy situs. (b) Medialization of the right tonsil using the Maryland bipolar forceps. Mucosal incision in the area of upper tonsil pole using the monopolar cautery instrument. (c) Dissection of the right tonsil along its capsule using the monopolar cautery instrument. (d) Post-tonsillectomy situs.
Postoperatively, the patient was monitored on the ENT ward and discharged home in good general condition. The histological examination confirmed the benign nature of both palatine tonsils with signs of chronic inflammation.
Discussion
Tonsillectomy is one of the most frequently performed operations in the world. In the USA, >100 000 tonsillectomies are performed every year [6]. The use of TORS for tonsillectomy is not new. It was first described in 2007 in the context of a radical tonsillectomy with an earlier da Vinci model in the USA [7] and has since been further improved. However, as the da Vinci SP system was only approved in Europe this year, clinical implementation in the field of ENT medicine is still in its infancy. The application of the da Vinci SP system in ENT medicine appears promising from our point of view. It enables high-precision access to narrow anatomical regions such as the tonsils, the base of the tongue or the hypopharynx with simultaneous high-resolution imaging. In our opinion, benign tonsillectomy is very well suited as an entry-level procedure for an experienced ENT surgeon to be able to safely use the da Vinci system for more complex procedures when such a system is established in routine clinical practice. In summary, we report on a technique for robot-assisted benign tonsillectomy using the da Vinci SP system. For the active application of the da Vinci SP system in ENT pathologies, e.g. head and neck tumors, further experiences should be shared and discussed.
Acknowledgements
We would like to thank Associate Professor Harishanker Jeyarajan, MD for his excellent surgical advice. We would also like to thank Professor Peter Grimminger (Department of General, Visceral and Transplant Surgery, University Medical Center Mainz) who arranged the surgical infrastructure for the implementation of the da Vinci SP system at our University Medical Center.
Conflict of interest statement
The authors declare no conflict of interest.
Funding
None declared.
Data availability
All data generated or analysed during this study are included in this article. Further inquiries can be directed to the corresponding author.
Consent
Written informed consent was obtained from the patient for use of images for academic and research purposes as well as publication.

{kind=link}
{kind=link}
{kind=link}