





Abstract
Venous thromboembolism (VTE) is a serious but rare complication of aesthetic surgery, with an incidence of 0.017% for liposuction and 0.01%–0.02% for augmentation mammoplasty. Despite the low incidence and appropriate patient selection, we present two cases of VTE in low-risk patients without hypercoagulability undergoing aesthetic procedures. In the first case, a 45-year-old woman with a history of anemia developed bilateral pulmonary embolism after ultrasound-assisted liposuction. In the second case, a 33-year-old woman with a history of oral contraceptive use developed deep vein thrombosis in the right upper extremity after augmentation mammoplasty. The patients were treated early and fully recovered after 12 months. This report highlights the importance of early diagnosis and treatment of VTE in aesthetic surgery, even in low-risk patients.
Introduction
Venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), remains a major concern for plastic surgeons because of its short-term mortality and long-term morbidity [1]. Although the exact incidence of VTE in aesthetic surgery is unknown, it is estimated to be ~0.09% and varies according to the procedure. Additionally, the specific risk factors for this patient population are not well documented [2]. Aesthetic surgery is generally considered to present a lower risk of VTE, since patients are usually healthy and more carefully selected for elective surgery. We present a case of bilateral PE after ultrasound-assisted liposuction and a case of upper extremity DVT (UEDVT) after augmentation mammoplasty.
Case presentations
Case 1
A 45-year-old woman with a history of anemia and a BMI of 20.1 kg/m2 presented with lipodystrophy of the abdomen, outer thighs, and inner knees. She was preoperatively evaluated and received an ASA I. Third-generation ultrasound-assisted liposuction, VASER (Sound Surgical Technologies, Colorado, USA), was performed under general anesthesia. Subcutaneous infiltration consisted of 1000 ml isotonic saline and 1 ml epinephrine 1/1000 infiltrated into the aforementioned lipodystrophic areas. Ultrasound was applied with a 3.7 mm probe at 80% amplitude in continuous mode. After emulsification, 1000 ml of fat and fluid were removed by traditional liposuction. The operative time was 130 min, and graduated compression stockings were used. On postoperative Day 6, the patient presented with respiratory distress, with an oxygen saturation of 96% and a heart rate of 105 bpm. Doppler ultrasound of the lower extremities showed no evidence of DVT, while chest tomography revealed bilateral PE (Fig. 1).
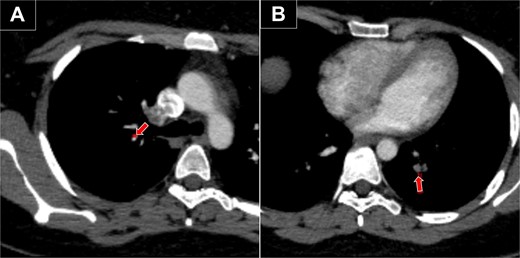
Chest CT with bilateral PE. (A) Embolism in the segmental artery of the right upper lobe (arrow). (B) Embolism in the posterior segmental artery of the left lower lobe (arrow).
Case 2
A 33-year-old woman with a history of oral contraceptive use and a BMI of 23.4 kg/m2 presented with breast hypoplasia. She was preoperatively evaluated and received an ASA I. A prepectoral augmentation mammoplasty was performed under general anesthesia. Même® MesmoMS® (Polytech Health & Aesthetics, Dieburg, Germany) 300-ml round implants were placed. The operative time was 80 minutes, and graduated compression stockings were used. On postoperative Day 7, the patient presented with pain, swelling, and erythema over the medial aspect of the right elbow and arm, with vital signs remaining normal. Doppler ultrasound revealed a right UEDVT (Fig. 2), and tomography showed thrombosis in the axillary and humeral veins (Fig. 3).
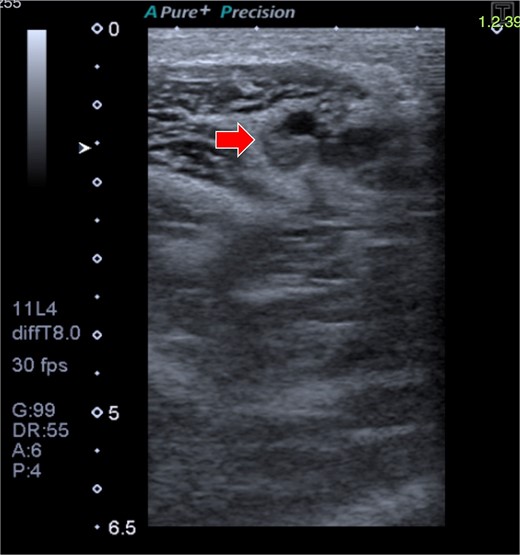
Doppler ultrasound shows DVT in the right axillary vein (arrow).
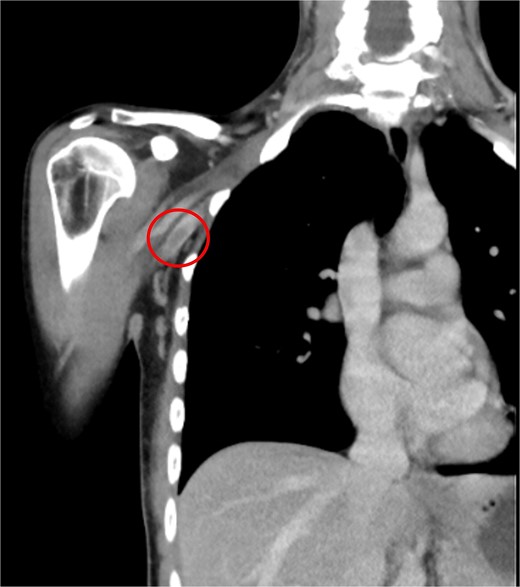
CT of the right upper extremity showing thrombosis of the right axillary and humeral veins (circle).
Both cases were treated with apixaban 10 mg/12 h for 7 days and then 5 mg/12 h for 6 months according to the American Society of Hematology guidelines [3]. In case 1, other investigations were performed to detect DVT (abdominal and pelvic CT; and Doppler echocardiogram), which were negative. Additionally, hypercoagulability tests were performed (protein C, S, antithrombin III, Leiden factor V, anti-cardiolipin IgG and IgM, anti-beta 2-glycoprotein IgG and IgM, lupus inhibitor), which were negative. After 7 weeks of treatment, we performed chest CT in case 1 and Doppler ultrasound in case 2, which confirmed resolution of VTE, and at 12 months of follow-up, the patients had complete recovery and good aesthetic results.
Discussion
VTE affects 1–2 people per 1000 each year in the United States. DVT most commonly occurs in the lower extremities, but the upper extremities are also affected [4]. Additionally, approximately one-third of patients with VTE have PE, with or without DVT [3].
Aesthetic surgery patients have a relatively low overall risk of developing VTE; among these procedures, body contouring has the highest incidence [2]. Liposuction is the most commonly performed aesthetic procedure worldwide [5]. Despite its popularity, it has complications, such as VTE, which occurs in 0.017% of cases [6]. Currently, only one case of VTE after ultrasound-assisted liposuction has been reported [7]. It involved a woman who underwent liposuction of 3050 ml of fat and fluid from the thighs and buttocks under epidural anesthesia with an operative time of 180 min. On postoperative Day 4, the patient was found unconscious in her bathroom. She did not survive. Autopsy revealed massive DVT in the lower extremities and bilateral PE. In our case, 1000 ml of fat and fluid were removed, and the operative time was shorter. Our patient developed bilateral PE without DVT. In addition, she progressed favorably, and other causes of VTE, including hypercoagulability, were excluded. We considered fat embolism and fat embolism syndrome (FES) as differential diagnoses [8]. In aesthetic surgery, fat embolism is mainly associated with liposuction and autologous fat grafting. However, our patient did not undergo these additional procedures and showed no clinical signs of FES, which usually includes respiratory distress, neurological symptoms, and petechial rash.
On the other hand, breast augmentation is the second most common surgical procedure worldwide [5]. The risk of VTE in a breast augmentation patient is 0.01%–0.02% [2, 9]. Approximately 10% of all DVTs occur in the upper extremities, and their incidence is increasing due to the growing use of medical devices [4]. To our knowledge, one case of UEDVT after dual plane augmentation mammoplasty has been described [10]. The patient developed DVT in the left axillary vein and massive bilateral PE. She required thrombolytic treatment with recombinant tissue plasminogen activator and aggressive anticoagulation with unfractionated heparin and warfarin, resulting in a left breast hematoma requiring drainage and removal of both implants. Finally, the patient was diagnosed with genetic hypercoagulability and refused to undergo further aesthetic procedures. Our patient underwent prepectoral mammoplasty and was monitored with a venous catheter in the right upper extremity and a padded sphygmomanometer in the left arm. She developed a right UEDVT without hypercoagulability and responded well to anticoagulation therapy with a full recovery and good aesthetic outcome.
Healthy patients undergoing elective aesthetic surgery do not yet have well-defined VTE risk factors, and there is no consensus on VTE prophylaxis in this population [11]. A study of 1254 aesthetic surgery patients showed that women older than 40 years, smokers, with 2 or more pregnancies, and those using hormone replacement therapy or oral contraceptives had a significantly increased risk of VTE [11]. Conversely, a prospective study of 1000 plastic surgery outpatients assessed with Doppler ultrasound before and after surgery showed that hormone therapy did not increase the risk of VTE [12].
Several risk assessment models (RAM) have been described to stratify patients according to VTE risk, but due to the lack of high-quality evidence and heterogeneity in the data, there is no recommendation regarding RAM that can be used for aesthetic surgery patients [13]. Based on our experience, we recommend individualizing VTE prophylaxis for each patient, considering their risk factors, the type of surgery, and the surgeon’s judgment [14, 15].
Although VTE is rare in liposuction and breast augmentation, it remains a significant public health issue. Many of the VTE prophylaxis strategies employed by aesthetic plastic surgeons are consistent with current literature and practice recommendations established by plastic surgery societies. However, despite these measures, the risk of VTE and its sequelae, such as post-thrombotic syndrome and death, cannot be completely eliminated [1]. Nevertheless, early recognition and treatment of these complications is crucial.
Conclusions
PE after ultrasound-assisted liposuction and UEDVT after breast augmentation are extremely rare. VTE should be suspected in patients who develop pain and swelling in the extremities or dyspnea after these procedures. This report highlights the importance of early recognition and treatment of VTE, even in low-risk patients without hypercoagulability undergoing aesthetic procedures.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}