





Abstract
Traumatic injury in children often involves traffic accidents, falls from height, bicycle accidents, abuse, and sports. We present our experience with a 6-year-old girl who bruised her abdomen by falling while running with a thermos bottle hanging diagonally across her neck and left shoulder, crossing in front of her body. After the injury, she was rushed to the hospital and plain abdominal computed tomography revealed free air, suggesting intestinal injury due to blunt trauma. She was transferred to our hospital, where abdominal examination revealed a bruise and redness at the umbilicus. There were signs of peritoneal irritation and guarding throughout the abdomen. Upright chest X-ray showed free air in the right subdiaphragmatic region. Laparoscopic inspection revealed one perforation and two serosal injuries. The damaged serosa was repaired, and the perforated intestine was resected and anastomosed. The patient was discharged on the 11th day following an uneventful postoperative course.
Introduction
Traumatic injury in children often involves traffic accidents, falls, bicycle accidents, abuse, and sports [1, 2]. When children incur abdominal trauma, the main sites of injury are the liver, kidney, spleen, and gastrointestinal (GI) tract. Radiologic modalities for assessing abdominal injury include ultrasonography and abdominal computed tomography (CT). However, CT at the time of injury often does not show obvious abnormal findings. If physical examination findings, blood test results, or clinical symptoms are worsening over time, radiologic reexamination is necessary [1, 2].
Case report
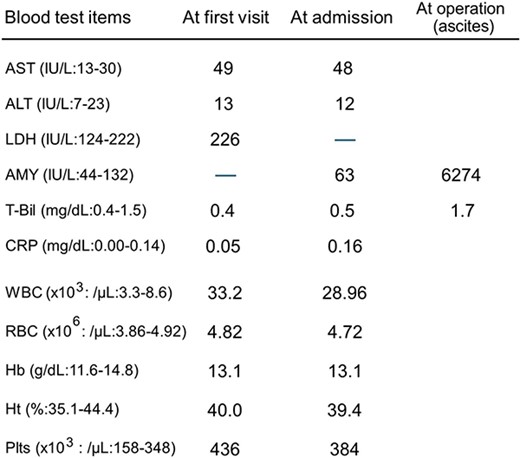
We present our experience with a 6-year-old girl who bruised her abdomen by falling while running with a thermos bottle (water bottle) hanging diagonally across her neck and left shoulder and crossing in front of her body. She went to school with a bruise on her abdomen, but 2 h after the injury she vomited and felt unwell; she was then rushed to the hospital. At the time of examination, her heart rate was 90 beats/min, her blood pressure was 110/62 mm Hg, her respiratory rate was 18 breaths per minute, her oxygen saturation was 98%, and her temperature was 36.6°C. Her abdomen was diffusely tender, but focused assessment with sonography for trauma was negative. She was kept for observation, but her symptoms did not improve. Plain abdominal CT was performed 3 h after the injury and revealed free air in the abdominal cavity, suggesting intestinal injury from blunt trauma. The whole pancreas was checked, but no obvious pancreatic injury was noted. Laboratory assessment showed a white blood cell (WBC) count of 33 200/μL, red blood cell (RBC) count of 4.82 × 106/μL, hemoglobin (Hb) of 13.1 g/dL, hematocrit (Ht) of 40.0%, a platelet count (Plts) of 436 × 103/μL, aspartate transaminase (AST) of 49 IU/L, alanine transaminase (ALT) of 13 IU/L, total bilirubin (T-Bil) of 0.4 mg/dL, and C-reactive protein (CRP) of 0.05 mg/dL (Table 1). She was transferred to our hospital 5 h after the injury. Abdominal examination on admission revealed a bruise and redness at the umbilicus (Fig. 1a), as well as diffuse signs of peritoneal irritation and muscular guarding. Upright chest X-ray showed free air in the right subdiaphragmatic region, but supine abdominal X-ray was normal (Fig. 1b and c). Laboratory assessment was repeated at our hospital and showed a WBC count of 28 960/μL, RBC count of 4.72 × 106/μL, Hb of 13.1 g/dL, Ht of 39.4%, Plts of 384 × 103/μL, AST of 48 IU/L, ALT of 12 IU/L, T-Bil of 0.5 mg/dL, amylase (AMY) of 63 IU/L, and CRP of 0.16 mg/dL (Table 1). Laparoscopic surgery was performed to assess the intestinal injury caused by blunt trauma. A transumbilical vertical incision was made, and the laparoscope was introduced. There were no apparent injuries of the liver and spleen, but there was bile leakage in the right upper quadrant, suggesting injury to the duodenum. However, further examination showed no injury to the duodenum and only the head of the pancreas was observed, but no damage was found. Bloody ascites was observed in the pelvis; biochemical analysis of the ascitic fluid revealed a T-Bil of 1.7 mg/dL and AMY of 6274 IU/L (Table 1). The small intestine was pulled out through the laparoscopic incision to confirm its integrity. There was no apparent injury on the ileocecal side, but there was a perforation on the oral side (Fig. 2a). The perforation was temporarily sewn, and the intestine was returned to the abdominal cavity. The site of injury was determined to be the jejunum, adjacent to the ligament of Treitz and two intestinal serosal injuries were also noticed (Fig. 2b). Two intestinal serosal injuries were repaired, and the perforated portion of the intestine was resected and anastomosed (Fig. 2c). After washing out the abdominal cavity, drains were placed under both hemidiaphragms and in the pelvis. The patient was allowed to begin oral intake on the sixth postoperative day. The drains were removed, blood testing was repeated to confirm return to normal values, and the patient was discharged on the 11th day following an uneventful postoperative course.
Laboratory analysis before and after admission.
 |
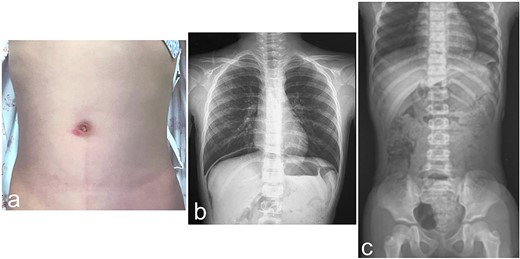
Physical and radiologic findings. (a) Abdominal photograph shows a bruise and redness at the umbilicus. (b) Upright chest X-ray shows free air in the right subdiaphragmatic region. (c) Supine abdominal X-ray shows no relevant findings.
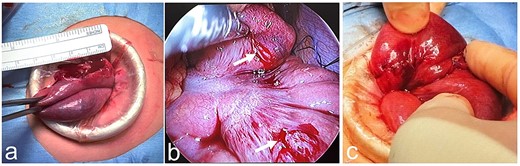
Intraoperative findings. (a) There is a perforation of the jejunum adjacent to the ligament of Treitz. (b) The perforation is temporarily sewn, and the intestine is returned to the abdominal cavity. Two intestinal serosal injuries are also noticed (white arrow). (c) Two intestinal serosal injuries are repaired, and the perforated portion of the intestine is resected and anastomosed.
Discussion
The Consumer Safety Division of the Consumer Affairs Agency of the government of Japan provides a warning for children: “Never run while carrying a water bottle or thermos bottle diagonally across the neck and shoulder in front of the body.” This warning was issued because there have been several reports of trauma caused by falling while running with a thermos bottle hanging in front of the chest [3].
Patient 1
A 10-year-old child fell while playing tag with a friend on the way to school; they had a thermos bottle or water bottle hanging diagonally in front of their body. The child developed abdominal pain and vomiting and was rushed to the hospital, where they underwent emergency surgery for peritonitis caused by damage to the small intestine.
Patient 2
A 9-year-old child fell and suffered a bruise on the abdomen while walking down a slope with a thermos bottle or water bottle hanging diagonally in front of their body. The child sustained a splenic injury but recovered with conservative treatment.
The Japan Pediatric Society issued an injury alert describing another patient [4].
Patient 3
A 7-year-old child was running to school and tripped and fell with a thermos bottle or water bottle hanging diagonally in front of their body. The child felt unwell, began vomiting, and was rushed to the hospital. Serum AMY and lipase were elevated, and abdominal CT showed rupture of the pancreatic body with disruption of the main pancreatic duct. Immediate laparotomy was performed, with irrigation and drainage. When the child continued to report abdominal pain, abdominal CT was repeated and the laparotomy incision was reopened due to leakage of pancreatic juice into the abdomen; the child underwent distal pancreatectomy and splenectomy due to pancreatic injury. After this reoperation, sudden bleeding was observed from the surgical drain. An emergent surgery revealed bleeding due to dissolution of the arterial ligation site caused by leakage of pancreatic juice. The artery at the bleeding site was ligated, and the child was discharged without further incident.
Another detailed account of traumatic injury caused by a thermos bottle or water bottle hanging diagonally in front of the body was published in the Journal of Abdominal Emergency Medicine [5].
Patient 4
An 8-year-old girl was running down the street with a water bottle hanging across her neck and left shoulder, in front of her body. She fell forward onto the water bottle and subsequently developed abdominal pain and frequent vomiting. She was taken to the hospital by ambulance. Contrast-enhanced abdominal CT suggested free air around the duodenum, and she underwent emergency laparotomy. A perforation in the descending part of the duodenum was repaired by simple closure, and the patient was discharged after an uneventful postoperative course. Injury to the GI tract from blunt trauma in children is uncommon (<1%). The majority of GI tract injuries are caused by a discrete point of energy transfer such as a seatbelt, a handlebar, or a blow from abuse [6]. Diagnosis of injury to the GI tract may be difficult and is often delayed. The incidence of duodenal injuries due to blunt trauma is 1–4%, and duodenal injury accounts for 0.2–3.7% of all trauma-related laparotomies. The diagnosis and management of duodenal injuries is often delayed [7]. Isolated jejunal perforation following blunt abdominal trauma is extremely rare. The majority of intestinal perforations are caused by traffic accidents, falls from height, or injuries from bicycle handlebars [8]. Previously, the author of this report described a patient who incurred a seat belt-induced jejunal rupture [9]. In that report, the AMY level in the ascitic fluid was elevated to 8757 IU/L, strongly suggesting intestinal injury.
Children are more likely to fall than adults and are less likely to reflexively support themselves with their upper limbs. When children are carrying water bottles, it is important that they put the bottle in a backpack and not run around with it hanging from their neck.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}