





Abstract
Tumors of the round ligament rarely happen; leiomyomas are considered the most common. Round ligament leiomyomas are benign tumors mimicking inguinal hernia, lymph nodes, or other inguinal masses. They are usually asymptomatic and take place in premenopausal female patients. This paper will present a case of a postmenopausal female patient who presented to our outpatient surgical clinic complaining of a right groin mass for 3 months. She was clinically diagnosed as a case of an irreducible inguinal hernia. After investigations, it turned out to be a round ligament leiomyoma, confirmed by the histopathological examination. There are broad differential diagnoses of inguinal masses. Although imaging exams could help diagnose leiomyomas, surgical excision followed by histopathological assessment is the best to confirm the diagnoses.
Introduction
The round ligament is considered the embryological equivalent of the gubernaculum testis in females. It is composed mainly of smooth muscle fibers that pass through the inguinal canal and extend from the uterus to terminate in the region of the mons pubis and labia majora [1]. Tumors of the round ligament are rare, but leiomyomas are the most common differential diagnosis whenever they exist. In the uterus, leiomyomas are the most frequent lesion, and they usually present as inguinal masses in premenopausal females [2]. Patients affected by this condition could be asymptomatic or present with vague symptoms. Due to their location, these lesions are often mistaken for hernias or lymph nodes [3]. However, apart from inguinal locations, abdominal and vulvar sites have been reported in the literature [4]. Surgical excision and histopathological assessment are the ways to provide the final diagnosis [5]. In this article, we report a case of a 57-year-old female patient who presented with a right groin mass for 3 months. After surgical excision and histopathological assessment of the specimen, she was diagnosed with a case of leiomyoma mimicking an inguinal hernia.
Case presentation
A 57-year-old postmenopausal female patient, a smoker, presented to the outpatient surgical clinic complaining of a right groin mass that was noticed ~3 months before presentation. The mass gradually progressed in size, was painless, and was associated with on and off-skin numbness. The patient denied any history of chronic cough, constipation, or exogenous cortisone use. She denied any weight loss, nocturnal fever, or urinary symptoms. Her past medical and surgical history was insignificant. The family history was unremarkable as well.
Physical examination revealed an overweight patient with normal vital signs. The local exam for groins was asymmetric in the standing position. A bulging mass was visible in the right inguinal area with no surrounding skin changes. Upon palpation, a 3 × 4 cm round, firm, painless subcutaneous mass felted with no overlying skin changes. The bulge was only partially reducible with the equivocal cough impulse. No other mass was appreciated in the same inguinal area or the other side. A working diagnosis of an irreducible right inguinal hernia was made, and the patient was scheduled for abdominal ultrasonography (US).
The US image revealed a well-defined hypoechoic heterogeneous echotexture mass lesion measuring 4.1 × 2.7 × 3.5 cm in the right inguinal area, with minimal peripheral vascularity in color flow Doppler. An adjacent normal inguinal lymph node was seen (Fig. 1).
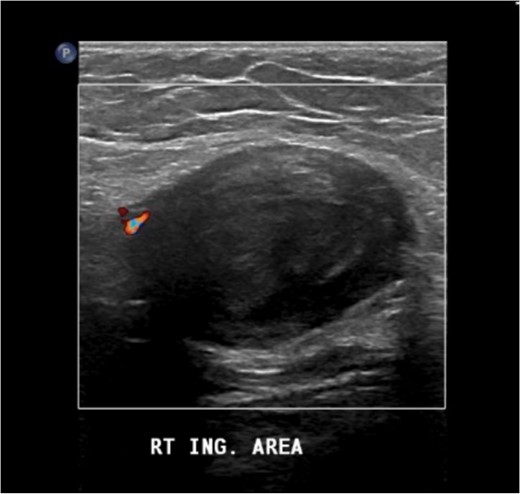
The US image revealed a well-defined hypoechoic heterogeneous echotexture mass lesion seen in the right inguinal area.
Further assessment by enhanced computed tomography (CT) of the abdomen and pelvis showed a heterogeneously enhanced, well-defined lesion in the right inguinal canal with no surrounding fat stranding or lymphadenopathy. The result corresponded to a hypoechoic lesion seen on the ultrasound with a lamellated appearance, suggesting a nerve sheath tumor or other tumors related to the round ligament, such as leiomyoma/fibroma (Fig. 2). The magnetic resonance imaging (MRI) showed an enhancement and solid lesion in the right inguinal area (Fig. 3).
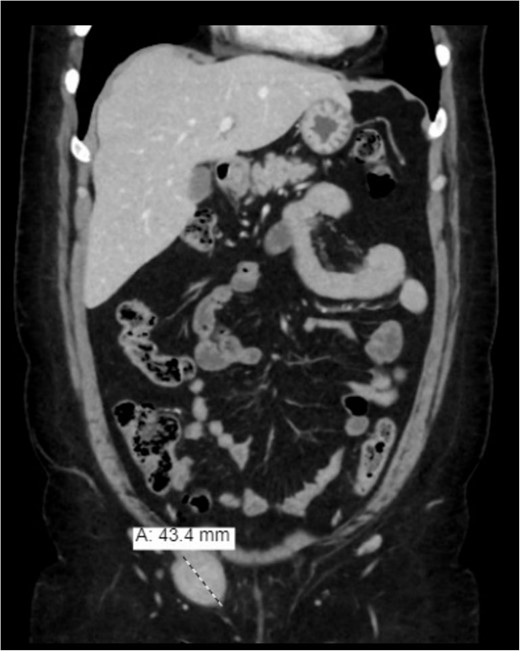
Enhanced (CT) of the abdomen and pelvis was done, and it showed a heterogeneously enhancing well-defined lesion in the right inguinal canal.
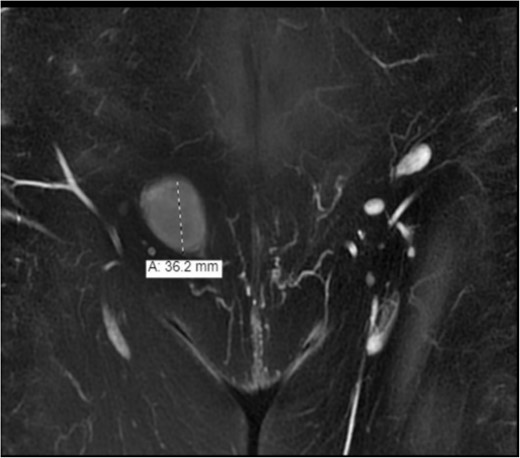
The MRI showed an enhancement and solid lesion in the right inguinal area.
The patient planned for mass excision. Intraoperatively, a transverse incision was made parallel to the inguinal canal in the right inguinal area. No hernial sac was identified; however, a well-shaped circular lesion ~3 × 3 cm in diameter was found just beneath the Scarpa’s layer with an attached cord-like structure going deep through the abdominal wall layers, most likely a remnant of the round ligament (Figs 4 and 5).

Well-shaped circular lesion found just beneath the Scarpa’s layer.

The picture shows the lesion with an attached cord-like structure going deep through the abdominal wall layers, most likely a remnant of the round ligament.
The mass was excised completely and sent for histopathology assessment. The histopathology assessment of the specimen revealed a benign smooth muscle neoplasm that was well-circumscribed and composed of interlacing bundles of benign spindle cells separated by collagen; there was no necrosis nor hemorrhage (Fig. 6). The spindle cells in the lump were positive for smooth muscle actin and Desmin (Fig. 7) but negative for s-100, consistent with leiomyoma diagnosis. The patient tolerated the surgery well, had an uneventful recovery, and was seen during follow-up patient was in good condition, with no active complaint.
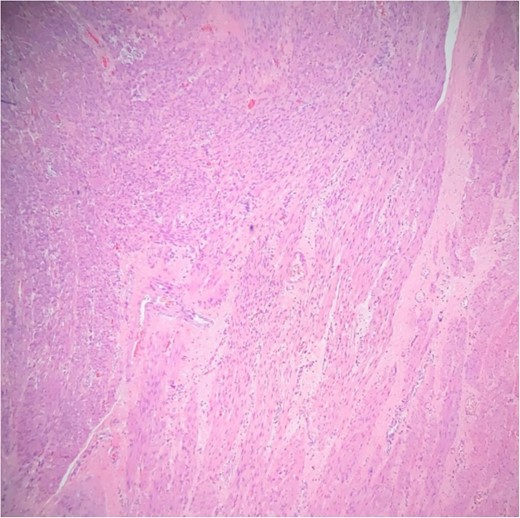
Interlacing bundles of benign smooth muscle cells, separated by collagen bundles.
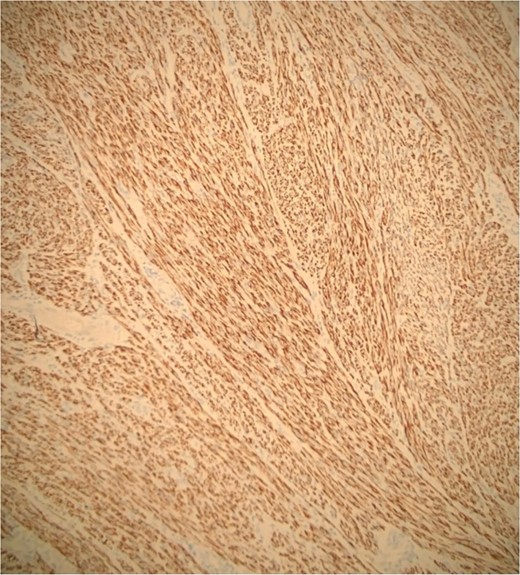
Diffuse positivity for desmin.
Discussion
Tumors of the round ligament of the uterus are rare and not frequently found. Leiomyomas are the most common histological tumors found in round ligament tumors, followed by endometriosis and mesothelial cysts [6, 7]. However, an incarcerated leiomyoma of the round ligament mimicking an inguinal hernia is a rare condition, and only a few cases have been reported in the literature [8]. Approximately one-half to two-thirds of leiomyomas occur in the extraperitoneal portion of the round ligament. Mass lesions that involve the extraperitoneal portion of the round ligament can mimic an incarcerated inguinal hernia or inguinal adenopathy as it passes through the inguinal ligament course [9]. The growth of leiomyomas is mainly promoted by estrogen, so they are known to be estrogen-sensitive due to the presence of estrogen receptors on the smooth muscle cells [10]. Therefore, estrogen replacement therapy is considered one of the risk factors for their development and growth. Other risk factors include age, obesity, early menarche, late menopause, and nulliparity [8].
Patients affected by leiomyomas are often asymptomatic, and their only complaint is inguinal swelling. Inguinal hernia is the most common differential diagnosis of this condition. Still, other differentials should be taken into consideration, such as femoral hernia, lymphadenopathy, femoral artery aneurysm, psoas abscess, hydrocele of canal of Nuck, leiomyosarcoma, and endometrioma [7]. Due to the broad list of differential diagnoses, preoperative imaging techniques such as regional ultrasound, enhanced CT-scan, and MRI are somehow helpful in reaching the diagnosis of leiomyomas [3, 11]. On CT with contrast and MRI images, they appear as encapsulated heterogeneous masses associated with calcifications. However, these findings are nonspecific and do not lead to a specific preoperative diagnosis [12]. The diagnosis can be confirmed preoperatively through a fine needle or a core needle biopsy [13]. However, our patient was diagnosed by surgical excision and histopathological examination of the mass, which was considered the management of choice at that time [8].
Conclusion
Even though it is an infrequent condition, leiomyomas of the round ligament can be a possible etiology of the inguinal mass. They can be mistaken for an inguinal hernia or lymphadenopathy. Different imaging modalities, such as CT scan and MRI, could establish a working diagnosis. However, surgical excision of the mass is the appropriate treatment and provides an accurate diagnosis.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}