





Abstract
Scrotal hernias are common in the general population. Patients often present acutely reporting pain or sometimes with more severe symptoms if the hernia is strangulated or incarcerated. An 81-year-old man presented with left-sided iliac fossa pain with no other associated symptoms. On clinical exam, a left-sided non-reducible inguinoscrotal hernia was detected with no evidence to suggest strangulation. Imaging revealed a probable colorectal cancer with likely liver metastases. The patient went on to have open surgery to excise the tumour with clear oncological margins. Colorectal cancers contained within scrotal hernias are very rare occurrences. In this case, the surgeon had the advantage of preoperative images that identified the cancer. In some cases, this cohort of patients do not have such scans prior to surgery and the surgical team can be faced with a much more complex operation than anticipated.
Introduction
Inguinal and scrotal hernias are commonly seen in clinical practice and therefore consume a lot of heathcare resources [1]. The lifetime risk for developing an inguinal hernia for men is 27% and females is 3% [2]. Owing to the fact they can contain segments of bowel up to 10% is at risk of incarceration causing intestinal obstruction, strangulation, or infarction [3]. Up to 0.5% of inguinal hernial sacs contain malignancies [4].
Lejar’s classification of primary tumours in the hernia sac dichotomies into saccular and intrasaccular subtypes. Saccular tumours include those that are primary (e.g. mesothelioma) or metastatic directly involving the peritoneal sac itself; intrasaccular tumours involve organs inside the sac. The majority of intrasaccular tumours are of intestinal origin [5].
Overall, primary colonic tumours are rarely found within hernia sacs but of the cases that are reported, the most common site of malignancy is the sigmoid colon, and they tend to be present more frequently on the left [6].
Case report
This a case of an 81-year-old man who was referred to the emergency department with a one day history of left-sided left iliac fossa pain radiating from his abdomen into the inguinal and scrotal region. He had no associated urinary or gastrointestinal symptoms and denied any systemic complaints such as weight loss, fatigue, or change in bowel habit. All vital signs were within normal limits. His blood profile showed a mild hyperkalemia but nothing else of note.
On clinical examination, he had a reducible right inguinal hernia and a large left-sided inguinal hernia that extended into the scrotum (as seen in Fig. 1). The hernia contained bowel and had been present for a number of years previous. The left-sided hernia had never caused the patient any issues previously.
Preoperative image of tumour within the scrotum.
His background medical history included past unprovoked pulmonary embolism’s and atrial fibrillation for which he was taking warfarin. He had never undergone any surgeries previously and he had been encouraged not to undergo surgical repair of his aforementioned hernias due to his co morbidities, age, and the lack of any associated symptoms.
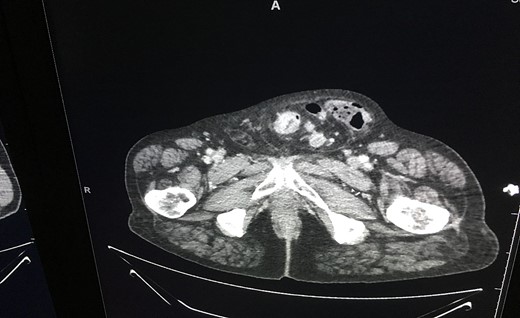
An ultrasound of the scrotum revealed ‘large left inguinal scrotal hernia containing omentum and bowel loops, on the right a high indirect inguinal hernia containing only fat tissue’ was described. A CT was subsequently performed, which revealed a likely primary sigmoid colon malignancy lying within the left-sided scrotal hernia and extensive liver metastasis (as seen in Fig. 2). The tumour contained within the hernia sac is illustrated in Fig. 3.

CT scan showing the tumour within the scrotum.
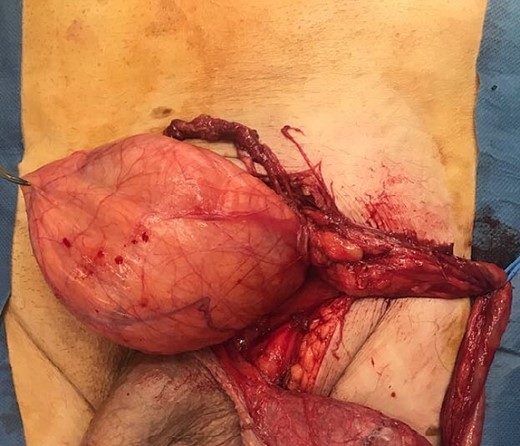
Intraoperative image of tumour within the hernia sac.
He was admitted to hospital after these investigations and his warfarin was replaced with therapeutic dose of subcutaneous enoxaparin. He had liver biopsy 4 days postadmission that confirmed metastatic disease. He was discussed at the multidisciplinary team (MDT) meeting and offered the choice of surgical intervention for his primary sigmoid tumour. After careful consideration, the patient chose the surgical option. He underwent open excision of the tumour (see Fig. 4).

Tumour postresection.
Postsurgery histology revealed adenocarcinoma and the patient went on to undergo systemic chemotherapy.
Discussion
Colon cancer contained within a inguinoscrotal hernia sac is a rare presentation. Clinical exam allows for the accurate diagnosis of inguinoscrotal hernias, but radiology or surgery is necessary to uncover the exact contents of the hernia.
This case emphasizes the important role of imaging as an adjunct to diagnosis and aid to preoperative planning. In the absence of imaging, a surgical team could be faced with a far more challenging operation than expected as the cancer would not have been identified pre op. A hernia repair that has the potential to turn into a cancer resection needs appropriate surgical expertise present at the time of the operation in order to manage the case appropriately.
In this case, a preoperative CT scan allowed for discussion at the MDT meeting and appropriate planning prior to the operation to be undertaken. Furthermore, the radiological diagnosis allowed this particular person to weigh up all options preprocedure. Ultimately, it is of the utmost of importance that a patient should be involved at every step of his/her treatment journey so the more information they can be given to guide their decisions, the better the outcomes.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}