





Abstract
Spontaneous hemorrhage within thyroid nodules is infrequent and challenging to manage. Patients with this condition typically manifest acute neck pain, swelling, and discomfort. This report details a rare case of a 49-year-old male patient who was not known to have any history of thyroid disease. He presented with a distinctive clinical scenario of a spontaneous hemorrhagic thyroid nodule that was managed surgically and had a satisfying outcome. In addition, we have conducted a review of the literature regarding the clinical presentation, diagnosis, and outcomes of published cases in correlation with our discussed case.
Introduction
Hemorrhagic thyroid nodules, a rare entity in the realm of thyroid disorders, have been documented in only a limited number of cases [1–4]. While certain predisposing factors are identified in the literature, it is crucial to emphasize that the specific etiology of the spontaneous hemorrhagic thyroid nodules remains largely unknown [5]. In contrast to provoked cases, where identifiable risk factors are at play, this spontaneous variant is notably scarcer, with only a scant number of documented instances in the literature [6, 7]. Thyroid nodules are relatively common and mostly benign, comprising a significant proportion (24.83%) of thyroid disorders [8]. Spontaneous hemorrhage within these nodules is comparatively infrequent occurrence. This is often accompanied by clinical indicators such as acute neck pain, swelling, and discomfort in affected patients [1]. In this report, we describe a rare case with unknown history of a thyroid disease presented with a unique clinical scenario of spontaneous hemorrhagic thyroid nodule. We also provided a comprehensive review of clinical presentation, diagnosis, and outcomes of similar cases reported in the literature (Table 1).
Case presentation
A 49-year-old male presented to the Emergency Department with a left neck swelling that had been rapidly increasing in size over the past 8 days (Fig. 1). He also experienced mild dysphagia to solids and dysphonia, a form of mild hoarseness. There were no other associated symptoms such as stridor, odynophagia, trismus, torticollis, shortness of breath, tachypnea, or constitutional symptoms like fever, night sweats, loss of appetite, and unintentional weight loss. He denied any history of recent upper respiratory tract infection or contact with sick patients. The patient’s medical history was only significant for an allergy to aspirin, with no recent consumption. He denied having any symptoms or a prior diagnosis of hypothyroidism or hyperthyroidism.

The reported patient with left neck swelling. (A) Anterior view. (B) Lateral view.
Upon examination, the patient was breathing on room air, hemodynamically stable, not in respiratory distress, and afebrile. Neck examination revealed a large anterior left neck swelling that was firm in consistency, non-tender, with no skin changes and no palpable lymphadenopathy. A flexible nasopharyngolaryngoscopy showed mild left lateral hypopharyngeal fullness with a normal view of glottis and bilateral mobile vocal folds with signs of laryngopharyngeal reflux. Cranial nerves examination was unremarkable.
Laboratory investigations showed a normal basic profile and normal thyroid function tests. An urgent contrasted computed tomography (CT) of the neck revealed a large left complex solid and cystic thyroid lobe lesion, measuring 6 × 6.6 × 10.3 cm, with retrosternal extension, exerting a mass effect on the trachea causing a shift to the right side. Multiple hyperdense nodularities were seen within the lesion, which could represent intralesional blood products, calcification, or active extravasation. The hyperdense component was evident on contrasted soft tissue window but not on the bone window, suggesting a hemorrhagic thyroid nodule. The lesion abutted the left common carotid artery with lateral displacement and compression of the left jugular vein. No suspicious necrotic lymphadenopathy, central airways patent, and no destructive bone lesions were appreciated (Fig. 2).
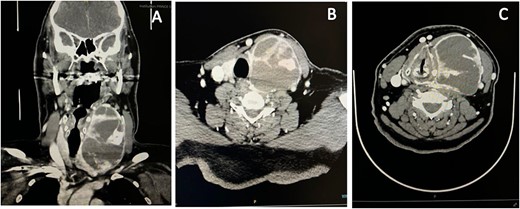
Neck CT scan revealed diffusely enlarged complex cystic and solid thyroid nodule compressing the trachea causing shift to the right side. (A) Coronal view. (B, C) Axial view.
The patient was admitted for observation and underwent ultrasound-guided aspiration by interventional radiology, which showed a 110 ml aspirate of dark blood with immediate improvement of patient’s symptoms of dysphagia and dysphonia (Fig. 3). Fine needle aspiration (FNA) was done later during his hospital course and was consistent with a Bethesda II benign lesion. The patient was discharged home in good condition and scheduled electively for thyroidectomy the following week. The need for surgical intervention was offered and explained to the patient due to the large thyroid nodule in a male patient and decreased sensitivity of FNA in multinodular large goiter. The benefits and risks of the procedure were thoroughly explained. After obtaining the patient’s consent, he underwent left hemithyroidectomy. The patient tolerated the procedure well with a smooth recovery and was subsequently discharged without any complications.

Ultrasound-guided aspiration by interventional radiology which showed a 110 ml aspirate of dark blood.
Histopathology revealed the presence of a heterogeneous cystic lesion with blood clots throughout the entire organ. The lesion weighed 253 g, measuring 10 × 8 × 6 cm. The outer surface appeared smooth, gray, and nodular, with an intact capsule. Hence, a diagnosis of a benign multinodular goiter was established. The patient was symptom-free at the postoperative follow-up appointment, without any recurrence of symptoms or lesions.
Discussion
A hemorrhagic thyroid nodule is considered a rare pathology. The exact etiology of spontaneous hemorrhage within these nodules remains uncertain, with proposed mechanisms including blunt trauma, chronic anticoagulation use, and bleeding following FNA [1–4].
In addition to the factors mentioned, a noteworthy factor that may contribute to spontaneous hemorrhagic thyroid nodules specifically is arteriovenous shunting, a condition that redirects blood at elevated pressure from arteries into the venous system within the nodule, leading to extravasation of blood. Activities or situations that raise intravenous pressure, such as strenuous physical exertion, episodes of coughing, straining during defecation, or the Valsalva maneuver, have the potential to induce vessel ruptures within the thyroid nodule, resulting in spontaneous bleeding [5].
As an example, Cerna et al. reported a rare case of a 64-year-old male who presented with breathing difficulties. Investigations revealed the presence of an arteriovenous malformation in the left lobe of his thyroid gland, measuring 8 × 7 × 5.5 cm. This malformation situated retrosternally caused deviation of the trachea to the right. The patient’s treatment involved a two-step approach; a radio-interventional procedure to disrupt the blood supply to the affected lobe of the thyroid and a left lobectomy with a partial sternotomy technique. Subsequent histological examination of the removed tissue confirmed that the arteriovenous malformation was benign in nature [11]. Nevertheless, our patient exhibited none of these predisposing risk factors.
Another illustrative case highlighted by Szeto et al. featured a healthy 36-year-old male undergoing elective nasal surgery, who developed an enlarging neck mass, an 8 × 6 cm right neck swelling that shifted the trachea to the left immediately after endotracheal intubation. Further investigations through on-table ultrasonography showed a ruptured thyroid cyst, identifying intubation as the causative factor of rupture [12].
In a retrospective cohort study conducted by Covino et al. between 2009 and 2018, a total of 59 patients out of 631 129 adult patients were identified as having hemorrhagic thyroid nodules. The mean age of these patients was 48.3 years, and there was a higher prevalence of females among the affected individuals. The main symptoms reported by the patients upon presentation were acute neck pain or swelling in 36 (61%), dysphagia in 17 (28.8%), dyspnea in 6 (10.2%), and other in 12 cases (20.3%). Four patients were on oral anticoagulant therapy. Among the patients, approximately half (50.8%) had a multinodular thyroid disease, while the remaining 29 had a single thyroid nodule. Thyroid surgery was performed on seven patients (11.8%), with only one case requiring urgent surgery. Final histological analysis revealed that four patients (6.8%) had a benign disease, while three patients (5.1%) were diagnosed with differentiated (papillary) thyroid carcinoma [1]. Our case bears similarities to this study in several aspects, including age, presenting symptoms, and the necessity of elective thyroidectomy. However, in our case, the patient was male and had no prior diagnosis of any thyroid-related conditions. Subsequent pathological report confirmed the presence of benign multinodular thyroid disease in our patient.
Radiological imaging plays an important role in the diagnosis of spontaneous hemorrhagic thyroid nodules. Yang et al. conducted a retrospective study involving 101 patients diagnosed with benign partially cystic thyroid nodules (PCTNs) between 2017 and 2019. Within this group, 59 patients experienced spontaneous intranodular hemorrhage. The study’s primary objective was to identify radiological factors that predispose these nodules to hemorrhaging. Their significant findings revealed that PCTNs with a rich blood supply were 2.8 times more susceptible to hemorrhage. Additionally, nodules with non-smooth margins within the solid portion had a 1.02-fold increased likelihood of hemorrhage, while those with spongiform internal content were 1.9 times more prone to spontaneous intranodular hemorrhaging [13].
In the majority of cases, patients with spontaneous hemorrhagic thyroid nodules typically do not require an urgent thyroidectomy. Instead, a carefully planned elective thyroidectomy or lobectomy guided by neuromonitoring is considered the most favorable and the mainstay treatment for spontaneous hemorrhagic thyroid nodules [4]. However, it is important to note that this condition can also be managed conservatively, as demonstrated in a case reported by Chan et al. involving a 93-year-old woman [6]. Her diagnosis was consistent with thyroid cyst hemorrhage on a CT scan. In their case, the patient was treated with needle aspiration then admitted for observation with intravenous hydrocortisone injections, which effectively reduced the swelling. This example highlights that conservative management can be a viable alternative to surgical intervention in specific cases of spontaneous hemorrhagic thyroid nodules, offering a less invasive approach to treatment.
Managing this condition is of utmost importance due to the potential life-threatening complications and, in rare cases, even mortality if not promptly addressed. The case report published by Dell'Aquila et al. serves as a poignant example of the potential severity of this condition. In their study, an 81-year-old female presented with a spontaneous hemorrhagic thyroid nodule and experienced acute respiratory distress, requiring urgent intervention. Unfortunately, the patient’s condition deteriorated due to the massive expansion of the hematoma, leading to tracheal compression and eventual death [7]. Furthermore, a case reported by Thirati et al. featured a 59-year-old deceased female who was admitted to the hospital with loss of consciousness during a hypertensive emergency. The subsequent autopsy revealed hemorrhagic stroke as the cause of death with intrathyroidal hemorrhage in a thyroid nodule causing airway obstruction [10]. These examples underscore the importance of timely and appropriate management for spontaneous hemorrhagic thyroid nodules to ensure favorable outcomes and avoid potential complications. Table 1 illustrates a comprehensive review of similar cases presented in the literature and includes the present case.
A review of literature on spontaneous hemorrhagic thyroid nodules
| 1st Author/ Year | Age (years) | Gender | Clinical presentation | Investigations | Histology | Management | Complications |
|---|---|---|---|---|---|---|---|
| Lee/ 2011 [9] | 73 | Male | -Tight heaviness -Hard swelling at the lower central neck region -Sudden dyspnea -LOC | Neck CT: a 6.5 × 5 cm homogeneous mildly enhancing cystic mass at the thyroid isthmus compressing the trachea | Nodular hyperplasia with no signs of carcinoma. | Emergency subtotal thyroidectomy | None |
| Chan /2012 [6] | 93 | Female | Hypopharyngeal swelling -Dysphagia & odynophagia -Non-productive cough. | -Flexible nasal scope and lateral neck x-rays -Urgent neck CT: bleeding into thyroid cyst causing tracheal deviation to right | Not done | -14 mL of old blood was aspirated. -Observation and IV hydrocortisone 200 mg | Residual bruising on anterior neck and chest |
| Wong /2016 [6] | 41 | Female | -Anterior neck swelling for 3 weeks’ duration. -Bruises over her anterior neck region and upper chest. -Intermittent dysphagia and odynophagia with change in voice | -Neck US: bilateral enlarged thyroid lobes with well-defined, lobulated hypoechoic solid cystic nodules (right 2.0 × 1.3 × 3.0 cm. left 2.8 × 2.4 × 3.6 cm) the left thyroid nodule had ruptured, causing mild neck hematoma. | Not done | Conservative management | None |
| Dell'Aquila/ 2019 [7] | 81 | Female | Acute respiratory distress | Autopsy: large thyroid gland in relation to the patient’s body mass (1510 g, in a patient of 142 cm and 45 kg). -Death was due to massive intra-thyroid hemorrhage causing acute external compression of the trachea. | |||
| Petersen/2021 [3] | Mid 80s | Female | Sudden collapse with expanding neck swelling | Not done | Microfollicular adenoma with significant bleeding | -Subacute left-sided thyroidectomy -Discharged after 3 days | None |
| Thirati/2022 [10] | 59 | Male | LOC in an episode of hypertensive emergency. | Autopsy: revealed hemorrhagic stroke as the cause of death and an incidental finding of intrathyroidal hemorrhage in a thyroid nodule. | Death | ||
| Basak/2023 [4] | 57 | Female | -Sudden onset of anterior neck swelling -Severe dyspnea -Loss of consciousness | -Blood gas analysis: severe acidosis -Neck CT: 6.2 × 5.3 cm mass from right thyroid lobe compressing trachea | Multinodular goiter with hemorrhage of cystic nodule | -Urgent drainage of hematoma with right lobectomy -Discharged on antibiotics | None |
| Alsalamah /2024 | 49 | Male | -Left neck swelling -Dysphagia & mild dysphonia | -Flexible nasal scope: left lateral hypopharyngeal fullness -Urgent neck CT: a large left solid and cystic thyroid lobe lesion, 6 × 6.6 × 10.3 cm, causing trachea shift to the right side. | Heterogeneous cystic lesion with blood clots, weighed 253 g & measuring 10 × 8 × 6 cm. -Diagnosis of a benign multinodular goiter | -Left hemithyroidectomy | None |
Conclusion
In summary, the occurrence of spontaneous bleeding within thyroid nodules is infrequent, and its exact origin remains unclear. Opting for elective thyroidectomy guided by neuromonitoring is a favored strategy in some reported cases, including ours. However, conservative management was favored by other authors. We confirm that prompt diagnosis and management are vital given the potential for severe complications.
Conflict of interest statement
None declared.
Funding
None declared.
Compliance with ethical standards
This research involves human participant(s) and/or animal(s).
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.

{kind=link}
{kind=link}
{kind=link}