





Abstract
Teratoma are germ cell tumors, most frequently arising in the gonads and retroperitoneal teratomas are rare, especially adrenal teratomas. Only a few case reports have been documented in the literature so far. We report the case of a 52-year-old asymptomatic male patient who had an incidental finding of a left adrenal teratoma during an abdominal computed tomography scan; due to the large size of the tumor, he underwent laparoscopic left adrenalectomy, and histopathological examination revealed a mature teratoma of the left adrenal gland, Patient recovering well after surgery and had no recurrence after 6 months of postoperative follow-up. The preoperative diagnosis of adrenal teratoma is challenging because imaging features are usually non-specific. Minimally invasive surgical resection is the best option for diagnosis and treatment of adrenal teratoma.
Introduction
Teratoma is a type of germ cell tumor originating from peripheral pluripotent stem cells, which composed of tissues from the ectoderm, mesoderm, and endoderm tissues. Teratomas are rare neoplasms with an incidence rate of 0.9 per 100 000 people [1]. It can occur at any age, and in adults it is mainly located in the gonads (testes or ovaries). Retroperitoneal teratomas are rare, accounting for only 4% of all primary teratomas [1–3], and adrenal teratomas are even less common. Because of their low incidence, our understanding of adrenal teratomas is still limited. Here, we report a primary teratoma of the left adrenal gland.
Case report
The patient was a 52-year-old male with a tumor in the left adrenal gland, measuring 7.2*7.5 cm, who had normal blood pressure and was in good health. He was admitted to the hospital for adrenal hormone examination, which showed normal adrenal function (renin: 2.34 pg/mL, aldosterone: 74.11 pg/mL, Adrenocorticotropic hormone: 35.20 pg/mL, cortisol: 243.0 nmol/L). Enhanced computed tomography (CT) of adrenal gland showed left adrenal region with rounded mixed density foci, with smooth margins, internal mature fat as the main focus, local mixed flaky slightly high density foci, and an internal “sac within a sac”, with a maximal cross-section of ~7.4*7.3 cm, with insignificant enhancement (Fig. 1), which was consistent with the manifestation of teratoma. The patient underwent laparoscopic adrenal tumor resection under general anesthesia, during the operation, the tumor was found to be closely adherent to the surrounding tissues, and the tumor was removed completely by blunt dissection with a peeling rod, and the patient’s vital signs were stable during the operation, and the tumor was incised under the table, which showed cystic solidity, with yellowish-white turbid contents, and hairy tissues were seen in the interior (Fig. 2A). Pathologic diagnosis was adrenal mature cystic teratoma (Fig. 2B) and the patient recovered well without any complications.
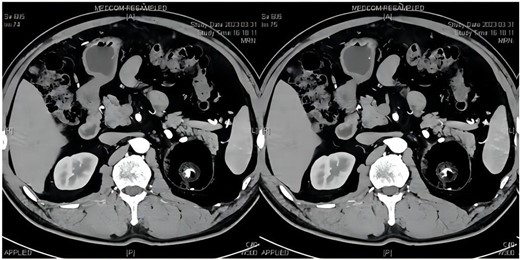
Adrenal gland CT: left adrenal gland huge tumor, size ~7.2*7.5 cm, internal fat mainly, see a “sac within a sac”, see calcification foci inside.
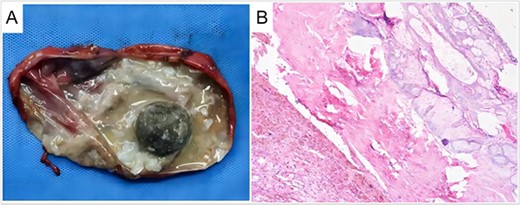
Macroscopic and microscopic picture of the tumor. (A) Tumor specimen. Calcification, hair, and lipid can be seen in the teratoma; (B) pathological examination (H&E staining). H&E, hematoxylin, and eosin.
Discussion
Teratomas are germ cell tumors composed of several different types of tissue. The tumors may be solid, unicystic, multilocular, or cystic-solid, containing hair, sebum, cystic fluids, calcifications, or teeth [4]. In adults, teratomas are frequently located in the gonads (testis or ovaries), 15% occurring in the extragonadal, 4% in the retroperitoneum, the adrenal gland is even rarer [5]. Here, we report a case of a primary mature teratoma in the left adrenal gland of a 52-year-old male.
Most patients with adrenal teratoma do not have obvious symptoms, and they are often discovered incidentally during routine radiological exams, Imaging plays an important role in the diagnosis of teratoma, and ultrasound can distinguish the cystic and solid components of the tumor, Using CT scans, the different tumor components, particularly fatty and bone-like tissue, can be identified, allowing for a more accurate diagnosis. Calcification, soft tissue, and compartmentalized structures are also common in adrenal teratomas. Calcification can be seen as speckled, plaque-like, striated, or cystic wall calcification. On enhancement scan, the soft tissue and peritoneum within the tumor showed enhancement [6]. The tumor of our patient showed fat, teeth, and cystic structures on CT, which favorably supported the diagnosis of teratoma.
It has been reported that 93% of teratomas contain a fatty component and 56% contain calcifications [7, 8], however, due to the diversity of imaging features of teratomas due to the differences in the components contained within them, the accuracy of CT scanning in detecting teratomas is only 64.3%, and retroperitoneal teratomas are easily confused with medullary lipomas, liposarcomas, pheochromocytomas, and angiomyosarcoma smooth muscle lipomas [9], which makes preoperative diagnosis difficult.
Surgical resection of the tumor is the preferred option for the diagnosis and treatment of adrenal teratoma, postoperative pathology can clarify the diagnosis [10, 11], and the prognosis is good after complete surgical resection, and the 5-year survival rate of patients is 100% [11, 12]. Compared with traditional open surgery, laparoscopic surgery has the advantages of less trauma, faster postoperative recovery, shorter hospital stay. Our patients were found to have severe intraoperative adhesions between the tumor and surrounding tissues, which greatly increased the difficulty of surgery.
Most retroperitoneal mature teratomas are benign. Tumor markers such as CA199, CEA, AFP, and HCG should be performed in patients with suspected retroperitoneal teratoma. So as to monitor the surgical treatment and recurrence of the tumor. Because retroperitoneal teratoma has the possibility of malignant transformation [11], close follow-up is recommended.
In conclusion, adrenal teratoma is extremely rare, and their preoperative diagnosis is challenging and relies on the imaging features of the teratoma, such as cystic mass, with mature fat and calcifications or teeth. Surgical resection is the method of choice for the diagnosis and treatment of adrenal teratomas, and postoperative pathology can clarify the diagnosis.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}