





Abstract
Appendiceal anomalies, particularly double appendices, are rare and mainly detected during non-appendiceal surgery in adults. Misrecognizing them can have serious consequences, both clinically and legally. It is critical that surgeons pay attention to the anatomical variations of the vermiform appendix, and always consider the possibility of duplicated appendix when diagnosing a right iliac fossa pain. Misdiagnosis can lead to life-threatening medical complications for the patient, with medico-legal implications.
Introduction
Appendiceal anomalies, in particular double appendices, are rare, with a reported incidence of 1/25 000 [1, 2]. This condition usually manifests itself during the first years of life, sometimes without apparent symptoms until adulthood. Despite their rarity, there are few documented studies on this subject. In this study, we present the case of a patient who underwent appendectomy and was admitted to the emergency department for appendicular syndrome with a computed tomography (CT) scan showing simple acute appendicitis.
Case presentation
A 27-year-old male complaining of abdominal pain was admitted to the emergency room. He had experienced pain in the right iliac fossa the day before, but had not reported any other digestive or extra-digestive signs at home. Clinical examination revealed a positive McBurney sign, and blood tests showed neutrophil-predominant hyperleukocytosis and increased C-reactive protein. An abdominal CT scan revealed a swollen latero-caecal appendix, containing two stercoliths at its base and a small fluid collection at its tip (Fig. 1). Appendectomy was performed, confirming the presence of two latero-caecal appendicular bases and two stercoliths. Both appendices were ligated individually (Fig. 2). A search for Meckel's diverticulum was negative. Histopathological examination confirmed the diagnosis (Fig. 3). The patient recovered without any complications.

Image of a 3D computed tomography reconstruction distinctly revealing two separate stercoliths, each located at a different site and oriented differently, thereby reinforcing the suspicion of appendiceal duplication.
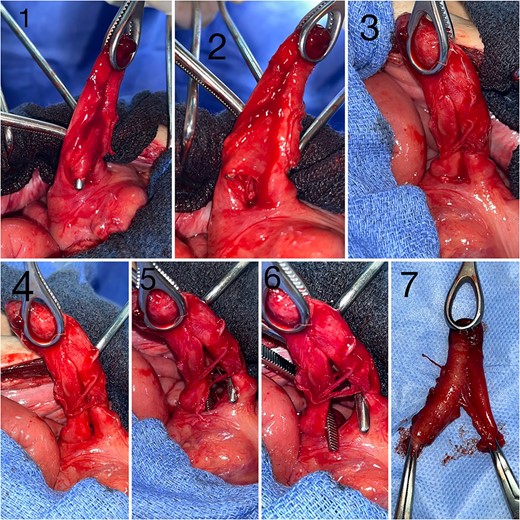
Intraoperative images depicting appendiceal duplication, 1 and 2: Images showing the two appendices, sharing a common mesentery, with two distinct bases and a common tip, 3 and 4: Images of the two appendices prior to dissection, 5 and 6: Images following the separation of the two appendices, 7: Surgical specimen.
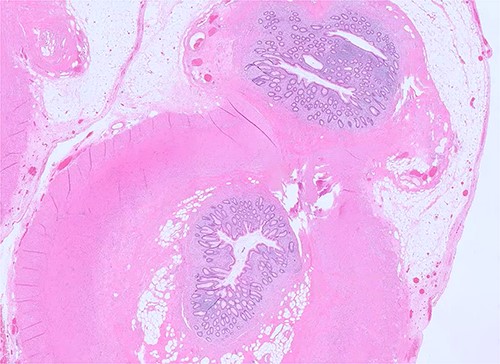
Microscopic examination of the specimen reveals two appendices with two separate lumens, partially sharing the muscularis layer, the sub-serosa, and the serosa (H&E, ×100).
Discussion
The first mention of a case of appendicular duplication goes back to 1892, thanks to the perceptive observations of Picoli [1–3]. This rare anomaly can manifest itself notably even in individuals of advanced age, as demonstrated by the case recorded by F. Calotã et al. in a patient aged 45 [4]. The classifications established by Cave in 1936 and Wallbridge in 1963, followed by the Cave-Wallbridge modification in 1993, laid the conceptual foundations for understanding these subtle anatomical variations [5, 6]. Interestingly, in 2010, Calotă et al. enriched this taxonomy by introducing the horseshoe-shaped appendix variant [7]. The observation we present here, highlighting a case of horseshoe-shaped appendix, is in line with the 16 similar cases documented in the literature [8]. In particular, it should be noted that this case is the second occurrence of this rare condition in the same hospital, the first having been the subject of a detailed analysis by Jabi et al.
Various hypotheses have been put forward as to the origin of this variation, including the theory of appendicular point fusion and that of mesoappendix division [9]. Diagnosis of this condition is frequently fortuitous, often occurring during surgery for other reasons, although radiology can sometimes lighten the path, as shown in the report by Liu et al. [7].
In our case, methodical surgical exploration confirmed the presence of a horseshoe-shaped appendix, with a single artery present in the mesoappendix. It is imperative to stress that careful inspection of the cecum is of paramount importance to prevent potential medico-legal complications in the event of subsequent inflammation of the residual appendix [10, 11]. The treatment of choice for this condition remains appendectomy, a procedure that can be performed either laparoscopically or by laparotomy, depending on the specific circumstances of the case [4, 5].
Conclusion
The mysteries of the appendix never cease to amaze, particularly with double appendices. This rarity, while spicing up medicine, reminds us of the imperative of acute clinical vigilance to prevent unexpected medical and legal complications in the context of right iliac fossa pain in adults.
Conflict of interest statement
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}