





Abstract
Benign peritoneal multicystic mesothelioma is a rare tumor of the visceral peritoneum. The authors present an atypical case of a 74-year-old man who presented with a multicystic mesothelioma of the ascending colon.
INTRODUCTION
Benign peritoneal multicystic mesothelioma (BPMM) is a rare tumor of the mesothelial layer of the visceral peritoneum [1]. They are among an intriguing group of primary tumors of the mesothelium including well-differentiated papillary mesothelioma, adenomatoid tumor and more aggressive diffuse peritoneal malignant mesothelioma. Due to dispute over the natural history and behavior of these lesions, the nomenclature is varied. Alternative names include multilocular peritoneal cyst or peritoneal inclusion cyst. They appear to exhibit female preponderance in younger women (30–40) of child-bearing age but can occur in men in up to 16% of cases [2].
Typically, they occur within the pelvis and are associated with previous surgery, endometriosis and pelvic inflammatory disease [2]. Findings may be incidental or patients may present with abdominal or pelvic pain with or without an appreciable mass [3].
CASE REPORT
A 74-year-old male construction worker presented with a 6 month history of right iliac fossa pain. He was otherwise fit and healthy with no significant medical history. He had one brother with Crohn’s disease but otherwise no family history of gastrointestinal or intra-abdominal pathology. He was an ex-smoker of 13 years with a heavy smoking history prior to this of 60 cigarettes per day.
A commuted tomography (CT) scan was performed in an outside institution, which demonstrated a 6.6-cm cystic mass between the sigmoid colon and caecum (Fig. 1). A subsequent colonoscopy yielded four small polyps, but the endoscope could not pass beyond the hepatic flexure. As the patient was minimally symptomatic, an interval CT scan was performed four months following initial presentation to re-assess the dimensions of the lesion. This showed no change in size with a persistent cystic mass in the right iliac fossa (Fig. 1). Following a lengthy discussion with the gentleman and his family regarding options including surgery versus a watchful wait approach with interval scanning, the patient chose to undergo elective resection.
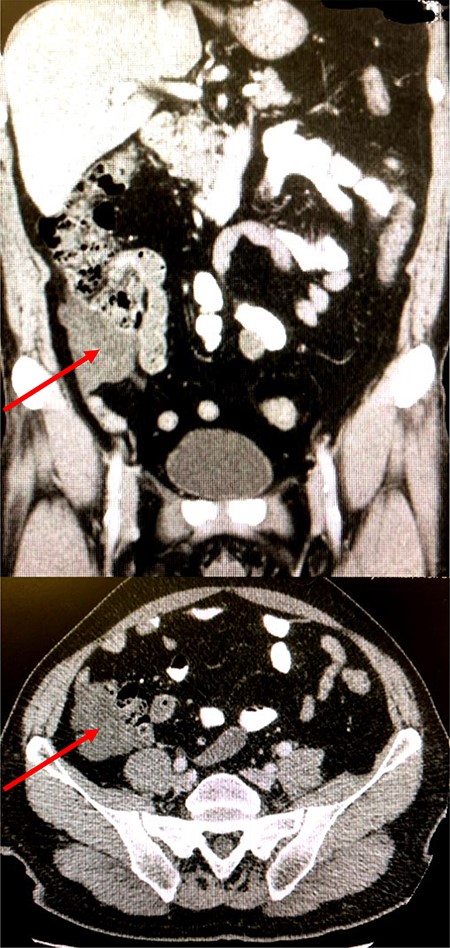
Coronal and axial CT images of lesion
The patient underwent an uncomplicated laparoscopic right hemicolectomy. Intra-operative findings were of a right ascending multicystic colonic mass consistent with imaging. The patient had an unremarkable post-operative course and was discharged home 5 days following his surgery. Histology revealed a 6 × 6 × 4.5 cm polycystic tumor with cysts ranging from <1 mm to 2 cm in size. About 21 lymph nodes were removed en bloc with the main specimen. Immunohistochemistry was performed, which was positive for mesothelial markers cytokeratin and calretinin, yielding a diagnosis of benign multicystic mesothelioma.
DISCUSSION
BPMM is a rare but recognized peritoneal tumor, first reported in 1979 by Mennemeyer and Smith [1]. There are <200 reported cases in the literature the majority of which are intra-pelvic tumors in women of child-bearing age [2]. To the authors’ knowledge, this is the second reported case of a right colonic presentation of this entity and the first of its kind in an elderly gentleman [4].
The etiology of this condition is poorly understood due to its rarity and thus debated. One school of thought affirms that the lesion is reactive, secondary to chronic inflammation, e.g. endometriosis, pelvic inflammatory disease and previous surgery. The rationale is that peritoneal fluid absorption is hindered as a result and becomes trapped within adhesions forming a cystic-like structure [5]. Potentially supporting the role of inflammation, an association has been proposed between BPMM and Familial Mediterranean Fever; an inherited disorder characterized by fever and intra-abdominal, thoracic and joint inflammation [6]. Other authors believe it harbors neoplastic etiology due to its slow but progressive growth pattern, high recurrence rate and rare but reported malignant transformation [7]. Reproductive hormones estrogen and progesterone have been implicated in its causality also; however, ER and PR receptors are inconsistently found at pathological examination [8].
BPMM may be diagnosed as an incidental finding or following symptomatic presentation with abdominal pain and/or a mass [2]. While radiological imaging can be a helpful guide, diagnosis is typically made at pathology [8]. The pathological classification of peritoneal mesothelioma can be confusing due to the varied nomenclature ranging from low malignancy potential to highly aggressive tumors such as diffuse malignant peritoneal mesothelioma. BPMM remains at the lower-risk end of spectrum but as previously mentioned, malignant transformation has been reported [7]. Percutaneous core biopsy may yield a pre-operative diagnosis of mesothelioma, but definitive subtype classification is normally made following surgical resection. The histopathological characteristics of BPMM comprise multiple cystic spaces characteristically lined by flat/cuboidal cells overlying a spindled stroma. They typically stain positive on immunohistochemistry for cytokeratin, calretintin, Wilms tumor-1 (WT-1) and negative for endothelial markers, facilitating distinction from other differential diagnoses including lymphangioma [8].
The treatment of BPMM is en bloc surgical excision due to its high recurrence rate and potential for malignant transformation [2]. In fact, these features have led many to argue that the term “benign” is a misnomer and should be abandoned. Hyperthermic intra-peritoneal chemotherapy (HIPEC) has been adopted in cases of malignant peritoneal mesothelioma following surgery to achieve complete cytoreduction [9]. This regimen has since been applied to cases of BPMM following surgery with the aim of minimizing recurrence and malignant transformation. Yan et al. [10] reported a series of 14 patients who underwent surgery and HIPEC for presumed pre-operative BPMM. About 11 patients demonstrated typical pathological morphology of which there were two recurrences over a median follow-up period of 64 months. This compares favorably to reported recurrence rates in other series of 30–50% but longer follow-up is warranted as some authors have documented recurrence decades after primary surgery [2]. Elucidation in a prospective multicentered trial setting is ideal but challenging given the rarity of this condition. Patients should nevertheless receive long-term follow up with some institutions advocating annual imaging surveillance. Due to the lack of unifying treatment and surveillance guidelines, this should be tailored to the individual.
CONSENT
Written informed consent was obtained from the patient for the publication of this case report with accompanying images.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES

{kind=link}