





Abstract
An incisional hernia (IH) is a common complication after a cesarean section (CS). Large IH mesh repair is problematic when initial fascial closure cannot be accomplished. We report the case of a large IH for 20 months after a CS with a midline vertical incision that was treated with a combination of modified peritoneal flap hernioplasty and abdominoplasty. There was a large fascia defect (15 × 21 cm) and adhesions of the omentum and the ileum to the anterior abdominal wall. CS with midline vertical incision, history of surgical site infections and obesity are risk factors that increase IH. In conclusion, this combination successfully repairs a large IH, reduces obesity, prevents recurrence and complications after hernia repair, improves the abdominal shape and patient quality of life. Abdominoplasty is also performed to create new umbilical and vascular preservation.
INTRODUCTION
One of the most complications after abdominal surgery including cesarean section (CS) is incisional hernia (IH). Several factors affected the development of IH such as age, infection, diabetes mellitus, obesity and smoking. Suture technique, material and incision location by the surgeon chosen also affect IH occurrence [1]. Previous studies found a strong association between the incidence of IH with CS [2]. Another study also found that a vertical midline shows a higher risk of developing an IH after a CS than a transverse incision [3].
The European Hernia Society (EHS) supports mesh implantation of hernia surgery to reduce the rate of recurrence [4]. Large IH mesh repair is problematic when primary fascial closure cannot be accomplished. Malik et al. have described the modified peritoneal flap hernioplasty (MPFH) that solves this problem [5]. A previous retrospective cohort study showed that the MPFH technique, when compared with the retromuscular sublay technique, had lower recurrence rates, especially for the repair of large IH [6].
Abdominoplasty is an aesthetic procedure that is one of the primary indications for skin and fascial laxity, which is commonly found in multiparous women, hernia and obesity. A combination of hernioplasty and abdominoplasty can be performed especially when associated with large-sized defects or divarication of recti, to achieve major quality of life improvement and superiority over hernioplasty alone in IH repair [7]. We report the case of a large IH after a CS with a midline vertical incision that was treated with a combination of MPFH and abdominoplasty.
CASE REPORT
A 25-year-old woman presented with an enlarged abdomen on the old surgical incision in the midline abdomen. Her medical history was a CS with a midline vertical incision in the second pregnancy 20 months before. Two weeks follow-up after delivery, she had a fever, severe abdomen pain and purulent discharge from the incision site. An ultrasound examination was performed, and she was diagnosed with surgical site infection (SSI) and endometritis. She was treated by surgical debridement, drainage, wound dressing and antibiotics. After recovery, she felt her stomach enlarge, especially when standing, but it shrunk when she lay down, and she felt distressed by the change in her stomach shape. The diagnosis of IH was established. Due to the coronavirus disease 2019 (COVID-19) pandemic, her hernia repair should be postponed.
The physical examination reports the patient’s height was 155 cm and weighed 65.7 kg with a body mass index (BMI) of 27.4 (obese), a scar on the midline of the abdomen (25 cm), an enlarged abdomen (25 × 30 cm) and a change in the position of the umbilicus (Fig. 1a). Routine laboratory blood analysis results were normal. Abdominal X-rays showed an IH, and there were no obstruction signs in the intestinal (Fig. 2). RT-PCR SARS-CoV-2 result was negative.
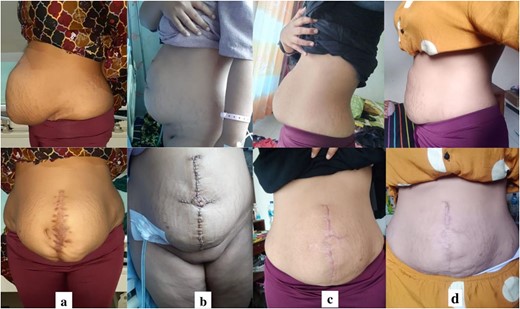
(a) Preoperative images; (b) postoperative images; (c) 3-month follow-up images; (d) 1 year’s follow-up images.
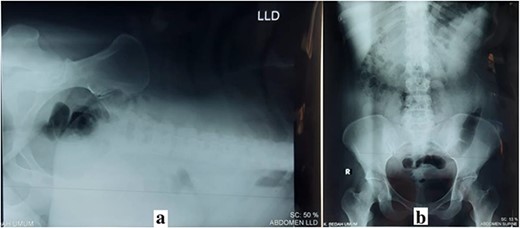
(a) Left lateral decubitus (LLD) abdominal X-ray; (b) supine abdominal X-ray.
The IH repair was performed with laparotomy. There was a large fascia defect (15 × 21 cm) and adhesions of the omentum and the ileum to the anterior abdominal wall. Adhesiolysis was performed to free the peritoneum from the surrounding fascia. MPFH with large polypropylene mesh insertion in the retromuscular (sublay) placement was performed to close the large defect of the IH and strengthen the abdominal wall. Abdominoplasty was performed by a plastic surgeon to remove excess skin and fat; create a new umbilical and close the entire abdomen (Fig. 3). She recovered completely and was discharged from the hospital 3 days after surgery. The patient was very satisfied and asymptomatic, and at 1 year of follow-up, the surgical scar was healing well (Fig. 1d).
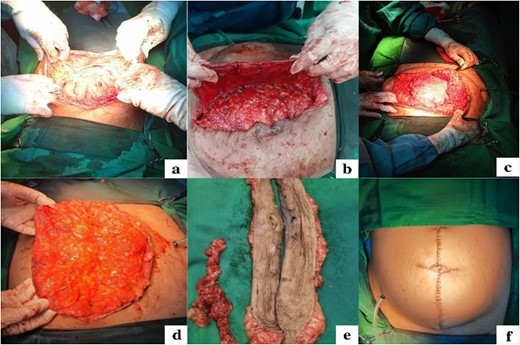
Intraoperative images. (a) Exploration and adhesiolysis release adhesion of the omentum and the ileum; (b) Close the large defect and strengthen the abdomen wall with MPFH; (c). Polypropylene mesh insertion with sublay placement; (d-e) Excision of excess skin including the navel; (f) Abdominoplasty to create a new umbilical and closure of the entire abdomen.
DISCUSSION
IH refers to the abdominal wall hernia at a previous surgical incision site. The EHS defines a large ventral hernia as a hernia with a defect longer than 10 cm [4] . In this case, the large IH was from a previous CS with a midline vertical incision in her second pregnancy. A previous study reported the rate of IH to be 0.0–5.6% after CS [8]. Two meta-analyses showed that the risk of IH is higher in a midline than in a transverse incision after abdominal surgery. The incidence of IH was 0–2.1% associated with a lower transverse incision and 3.0–20.6% with a midline vertical incision [3]. To prevent IH in a CS with a vertical midline incision, The National Institute of Clinical Excellence recommends using a small needle on a slowly absorbable suture in a continuous suture with a ratio of 4:1 for mass closure. Prophylactic antibiotics can prevent wound infection. In women at risk of IH due to having multiple cesareans, obstetricians should consider using slowly absorbable sutures such as Polydioxanone [2].
Two weeks after delivery, the patient was diagnosed with a SSI and endometritis that increased the risk of IH. SSIs are independent risk factors that significantly increase the risk of IHs [9]. The patient is also obese (BMI 27.4). Obesity has become an influencing factor both for IH and its complication. It is highly risky for incarceration and recurrence after repair. Another study of 700 cases found a significant association between IH and BMI. The occurrence of IH increased from 7.8% for individuals with a BMI of <24.4 kg/m2 to 18.8% for those with a BMI >24.4 kg/m2. Additionally, a multivariate analysis revealed that a BMI >24.4 kg/m2 was an independent predictive factor for IH incidence [10].
During the COVID-19 pandemic, EHS has recommended that elective abdominal wall surgery including hernia repair should be postponed [4]. Delayed hernia repair increased the risk of acute complications such as obstruction, incarceration, strangulation and complications caused by increasing hernia size [11]. In general, surgical techniques and materials do not change during a pandemic but COVID-19 infection risk and the patient’s clinical status shall be considered. However, some principles of abdominal wall surgery shall clarify and adopt certain techniques to minimize increased intra-abdominal pressure. The experts prefer the placement of extraperitoneal mesh and midline reconstruction over implementing intraperitoneal mesh [1, 4]. In this case, we used sublay mesh placement for the best treatment for the patients. Sublay was the most proper mesh placement option with the lowest probability 77.3% for SSI and 94.2% for recurrence [9].
The MPFH technique has been described before, and this technique uses hernial sac flaps to bridge the fascial gap and isolate the mesh from both the subcutaneous space and the intraperitoneal, utilizing the retro-rectus space medially and the avascular plane between the external and internal oblique muscles laterally (Fig. 4) [5, 12]. This technique prevents surgical site occurrence (SSO) such as post-operative hematomas, seroma and wound necrosis as it preserves periumbilical perforators. It results in less SSI and fewer intraabdominal adhesions after major hernia repair [13]. A retrospective single-center cohort study on 174 patients showed that the MPFH technique had a lower recurrence rate than the retromuscular sublay technique, and patients were more satisfied [12]. Another retrospective study in 251 patients with a large midline (68.1%) and lateral (31.9%) ventral hernias showed MPFH technique had a very low recurrence rate, safe and was associated with few complications [6].
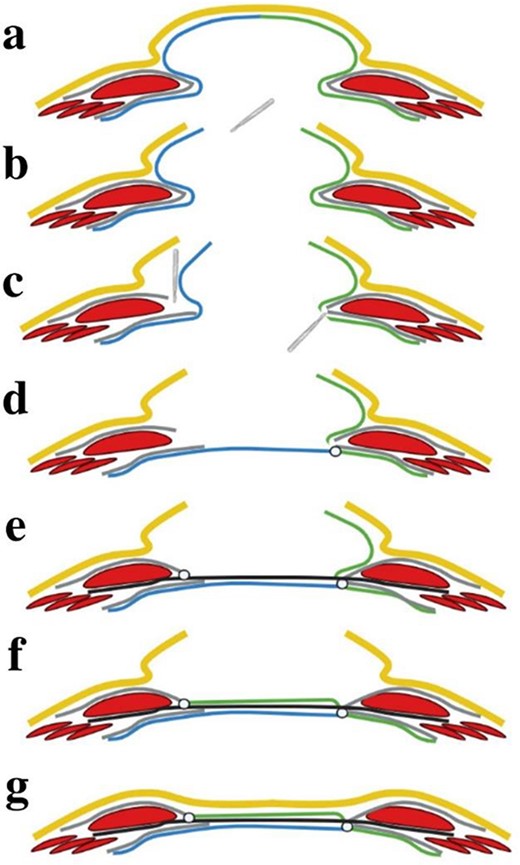
Schematic figure of MPFH technique: (a) The IH, the hernial sac left side (blue) and right side (green); (b) The skin (yellow) and the hernia sac are incised at the prior operative scar; (c) One anterior and one posterior flap are created by entering the retromuscular space through incising the left side’s anterior fascial sheath and the right side’s posterior fascial sheath; (d) The abdominal cavity is closed by suturing the posterior rectus fascia on the right side and the posterior flap. The rectus muscles are as closely approximated as possible; (e) The retromuscular mesh is placed and fixated by suture to the fascial margins. The anterior fascial sheet is sutured to the mesh as closely as possible to the midline; (f) The mesh is covered with the anterior flap which is sutured to the fascial margin on the left side; (g) Closure of the skin and subcutaneous tissue.
IHs are associated with excess skin and fat, laxity of muscle and abdominal shape deformity with hernia bulge scars. These changes have an impact on the physical and mental health of patients such as digestive disorders, back pain, urinary incontinence, eating disorders and an increased tendency to stress and depression. A combination of hernioplasty and abdominoplasty using a well-fixed retromuscular sublay technique is associated with low surgical site occurrence (SSO) including seroma, hematoma, and wound healing disturbances, and a durable improvement of abdominal shape and contour in both men and women. In addition, abdominoplasty in IH repair can improve the quality of life, hygiene, patient satisfaction in appearance, self-confidence and mental health of the patients [7].
One of the most important abdominoplasty procedures is umbilical vascular preservation. Simultaneous ventral IH repair with abdominoplasty has been demonstrated to put the umbilicus at risk of impairment or loss of blood supply. Large IHs can distort anterior abdominal wall anatomy and cause skin and soft tissue thinning. Careful intraoperative planning must determine the safe plane of dissection and point of entry of the hernia repair to avoid umbilical ischemia. This planning considers the location relevant to the umbilical stalk and the size of the hernia [14].
In conclusion, a CS with a midline vertical incision, a history of SSI and obesity are risk factors that increase IH. A combination of MPFH and abdominoplasty successfully repairs a large ventral IH, reduces obesity, prevents recurrence and complications after hernia repair, leading to an improvement in the abdominal shape and patient quality of life. Abdominoplasty can also can be performed to create a new umbilical and vascular preservation.
ACKNOWLEDGEMENTS
The authors thank Resdiyanto MD as a general surgeon that helps to manage operatives of the patient, the Department of Plastic and Reconstructive Surgery, and the Ethics Committee of Paru General Hospital, Jember, Indonesia.
CONFLICT OF INTEREST STATEMENT
The authors declare that there are no conflicts of interest regarding the publication of this article.
FUNDING
No funding was used in this study.
DATA AVAILABILITY
All the data are presented in the main manuscript. Additional supporting files are available for review and can be requested by the journal's editor at any time.
ETHICAL APPROVAL
Our study has been reviewed and approved by the Ethics Committee of Paru General Hospital, Jember, Indonesia. A copy of the ethical approval is available for review and can be requested by the journal’s editor at any time.
CONSENT
Written informed consent was obtained from the patient for the publication of this case report and accompanying images. A copy of the written consent is available for review and can be requested by the journal’s editor at any time.
References
Birindelli A, Sartelli M, Di Saverio S, et al. Update of the WSES guidelines for emergency repair of complicated abdominal wall hernias.

{kind=link}
{kind=link}
{kind=link}
{kind=link}