





Abstract
Few reports have described a submucosal tumor (SMT)-like colon tumor together with appendiceal cancer. Moreover, some appendiceal tumors may exhibit a cecal protuberance. Here, we report an uncommon case of appendiceal cancer with an SMT-like tumor, which was a protuberant lesion in the ascending colon. To our knowledge, this is the first report in Japan. Our case was a 50-year-old man with an ascending colon tumor presented at our hospital for further evaluation of this lesion. This was discovered as a cystic lesion near the ascending colon on colonoscopy. Our initial diagnosis was an ascending colon SMT-like tumor, and our treatment strategy was laparoscopic resection. The differential diagnosis was appendiceal cancer or mucocele. Postoperative pathological findings led to a diagnosis of adenocarcinoma of the appendix. The postoperative course was uneventful, and the patient was followed up with computed tomography and blood sampling on an outpatient basis.
INTRODUCTION
Primary appendiceal cancers are uncommon among patients with colorectal cancer [1], with malignant findings observed in a few cases of appendectomy (<1% cases) [2–4]. A submucosal tumor (SMT) is more common in the stomach and esophagus than in the colon [5]. Previous studies have reported the presence of SMT-like lesions in the cecum [6, 7]. However, our case presents a unique scenario, as to our knowledge, it is the first report of an ascending colon SMT-like lesion caused by an appendiceal cyst with diagnosed cancer after a surgical procedure.
CASE PRESENTATION
A 50-year-old man was examined at a local hospital for an annual check-up, and colonoscopy revealed an SMT-like lesion near the ascending colon. Due to this finding, the patient was referred to our hospital for further testing and treatment. He had no significant medical history or abnormal laboratory data, and physical examination findings were unremarkable. Colonoscopy confirmed the presence of SMT-like lesion in the ascending colon, while the cecum and Bauhin valve appeared normal. A cystic lesion in the intestinal wall was discovered on endoscopic ultrasonography (Fig. 1). Contrast-enhanced computed tomography (CT) also revealed the same lesion near the ascending colon, measuring 15 mm in diameter, with unclear continuity and no evidence of swollen lymph nodes (Fig. 2). Based on these findings, our preoperative diagnosis was an ascending colon SMT. Differential diagnoses included an appendiceal tumor and colon cancer. We planned to dissect the tumor for definitive diagnosis and treatment. However, endoscopic submucosal dissection is difficult for differential diagnoses.
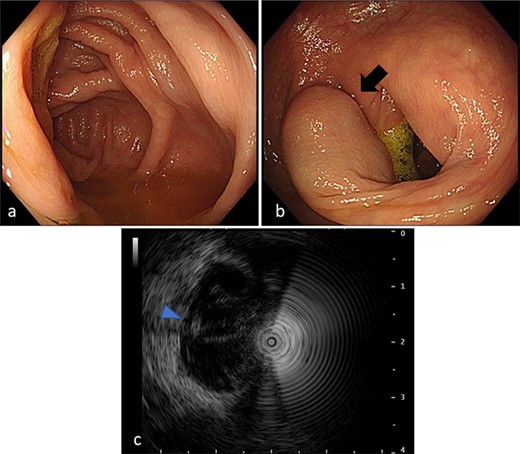
Colonoscopy findings. (a) Total colonoscopy revealing no mucosal changes in the cecum. (b) A tumor suggesting an SMT in the ascending colon (arrow). (c) Endoscopic ultrasonography revealing a cystic lesion (arrowhead) in the ascending colon.
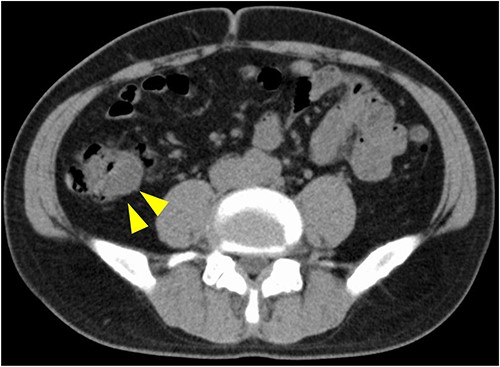
CT image. An iso-density lesion in the ascending colon (arrowhead).
The surgical procedure involved laparoscopic ileocecal resection. Intraoperatively, the appendix was not detected, and a part of the fatty tissue was adhered to the retroperitoneal organs (Fig. 3). Hence, en bloc resection of the right gonadal vein and retroperitoneal fat was performed. The operation lasted for 242 min, with a blood loss of 43 ml. The pathological findings showed a well-differentiated adenocarcinoma in the appendix, which was classified as well-differentiated adenocarcinoma, pT3N0M0, Ly1a, V0, Pn1a, PM0, DM0, RM0, pStage IIa, according to the Japanese Classification of Colorectal, Appendiceal, and Anal Carcinoma, 9th edition.
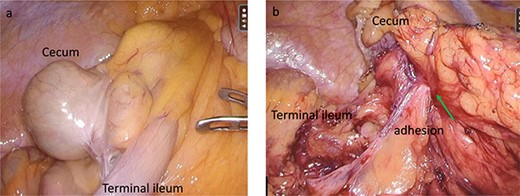
Intraoperative findings. (a) Surgical findings revealing an undetectable appendix in the cecum. (b) After mobilization and resection of the ileoceum, the lesion (arrow) is adhered to the retroperitoneum and the right gonadal vein.
Macroscopic findings revealed a dome-like elevation in the mucosal lumen and fatty tissue adhesion, with an undecidable appendix with the serosal lumen of the ascending colon (Fig. 4). The cut surfaces exhibited thickening of the appendiceal wall and a cystic region surrounding the appendix. However, microscopic analysis revealed invading malignant cells in the subserosal layer of the appendix and in the cystic lesions. This significant cystic lesion did not involve the muscle layer of the ascending colon. Moreover, cancer cells caused severe damage to a part of the appendiceal wall (Fig. 5). The postoperative course was uneventful, and no recurrence was observed during the outpatient follow-up.
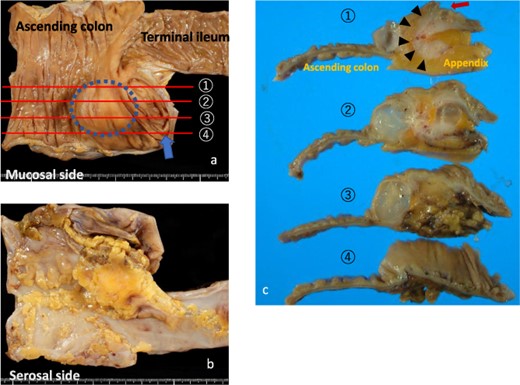
Macroscopic findings. (a) SMT-like elevation in the ascending colon (dotted circle). There are no mucosal changes in the appendiceal orifice (arrow). Each tissue has four slice lines. (b) Fatty tissue adhesion and undetectable appendix are noted on the serosal side of the specimen. (c) Formalin-fixed slices. Slice one shows the appendix surrounded by fatty tissues (arrowhead) and the appendiceal orifice (arrow). Slices two and three primarily show the cut surfaces of the cystic lesion.
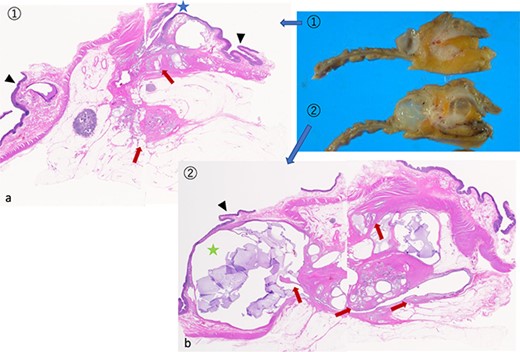
Microscopic findings of the sliced specimen. (a) Cancer cells invading the subserosal layer (arrow) in slice one. The appendiceal orifice (star) and cecal mucosa (arrowhead). (b) Slice two has a cystic lesion (star) with mucus production beneath the colonic mucosa (arrowhead) and cancer invasion (arrow). Note: Springer Nature remains neutral concerning jurisdictional claims in published maps and institutional affiliations.
DISCUSSION
Appendiceal cancer is considered uncommon, accounting for ~0.5% of gastrointestinal tumors [3]. The first diagnosis and symptoms often occur with appendicitis. Thus, the first procedure is frequently appendectomy. The percentage of preoperative cancer diagnoses is 14–22%, although appendiceal malignancy is often diagnosed alongside appendicitis [8]. In some previous reports, cancer has been found in ~5% of periappendiceal abscesses or appendicitis cases. However, there are some poorly defined features that are difficult to diagnose [9]. Enhanced CT assisted in distinguishing between malignant lesions and mucocele of the appendix [10]. This report describes the malignant potential of the appendix, indicated by the thickening of the appendix wall and soft tissues on CT. However, the appendiceal cancer in our case could not be effectively diagnosed with enhanced CT.
A dome-like elevation with smooth mucosa at the appendiceal orifice, known as the volcano sign, is a characteristic finding of appendiceal tumors on colonoscopy, but it was not found in our case [11]. Hence, there was an SMT-like finding in the ascending colon near the Bauhin valve during colonoscopy. Some SMT-like colon cancers, involving cell and tumor exposure to the mucosal surface on colonoscopies, have been reported [12, 13]. However, our case had neither changes in the mucosa nor smooth elevation in the lesion, resulting in an increased difficulty for accurate diagnosis.
In recent reports, additional colon resection for appendiceal cancer has been controversial. Appendectomy has been recommended in cases of mucosal cancer or no lymphovascular invasion on histology [14]. However, in the case of histologically diagnosed advanced cancer, additional ileocecal resection, right hemicolectomy, lymph node dissection and systemic chemotherapy have been recommended [15, 16]. Our case resembled the latter scenario, with malignant cells forming cystic lesions around the ascending colon. Hence, en bloc resection was an appropriate procedure. However, since no discrepancies with the preoperative diagnosis were observed, it was necessary to differentiate appendiceal cancer from ascending colon SMT-like tumors and choose the appropriate surgical method.
CONCLUSION
Herein, we report a rare case of appendiceal cancer. Since there are no previous reports on appendiceal cancer showing SMT-like lesions in the ascending colon, this report will assist in diagnosing a similar case of appendiceal cancer in the future. However, further research and accumulation of additional case reports are required to enhance our understanding of this condition.
ACKNOWLEDGEMENTS
We thank the members of the Department of Pathology for pathological diagnosis and detailed considerations in this report.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
AUTHORS’ CONTRIBUTIONS
All authors contributed substantially to the conception and interpretation of this report and data analysis. They also planned this report or critically revised it for important intellectual content. The authors have approved the final version of this manuscript for publication. They agreed to be accountable for all aspects of their work. All authors read and approved the final manuscript.
ETHICS APPROVAL
All procedures followed the 1964 Declaration of Helsinki’s ethical standards and subsequent amendments.
CONSENT FOR PUBLICATION
Informed consent was obtained from the patient.
DATA AVAILABILITY
Data sharing is not applicable to this article as no new data were created or analyzed in this study.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}