





Abstract
Foreign body in the anal canal may be inserted for sexual gratification or sexual assault or accidental or drug trafficking. We report a case of a male who accidentally inserted a cough syrup bottle in his rectum. Presentation is usually late due to fear and embarrassment. The manual attempt of removal may be tried under adequate anesthesia. Post-procedure sigmoidoscopy or colonoscopy may be helpful to diagnose laceration or mucosal injury.
INTRODUCTION
The rectal foreign body is a rare presentation at the Emergency Department. Whatever may be the motive whether it’s sexual gratification, concealment, body packers, sexual assault and, rarely, accidental the mortality and morbidity is high in the rectal foreign body as they only present for medical attention after several unsuccessful attempts to remove the object alone due to embarrassment. The standard technique for the trans-anal approach involves the combined use of analgesia, sedation, anesthesia and an attempt at manual removal of the foreign body. We hereby present a case of a male who was referred to the Emergency Department with a cough syrup bottle in his rectum. A 58-year female was admitted in emergency with a foreign body stuck in the anal canal for 24 h. He is a known case of psychiatric illness not under medication. It was acute in onset that happened while he was scratching his anal area with a cough syrup bottle. Following insertion, he developed severe pain and was unable to pass stool flatus; however, there was no per rectal bleed. He gives no history of past medical or psychiatric illness. His vitals were within normal limits and systemic examination was within normal limits. At emergency X-ray of the abdomen and pelvis was done, which showed a foreign body in the anal canal (Figs 1 and 2). Blood investigations were within normal limits. Digital rectal examination was done; however, no mass or foreign body was palpable. The patient underwent emergency manual removal of the foreign body via obstetric forceps under general anesthesia. Operative findings showed a foreign body (cough syrup bottle) of size 10 cm × 15 cm in the distal rectum about 8 cm above the anal verge (Fig. 3). The patient developed severe pain and stool incontinence and so was admitted at the ward and kept under observation. Psychiatric and cermatology consultation was done and the patient was discharged on the second postoperative day under oral medication. Sigmoidoscopy was done on a follow-up, which showed normal findings with minimal mucosal tear without perforation.

X-ray of abdomen and pelvis showing a foreign body at rectum.

X-ray showing abdomen and pelvis with foreign body with no signs of perforation.
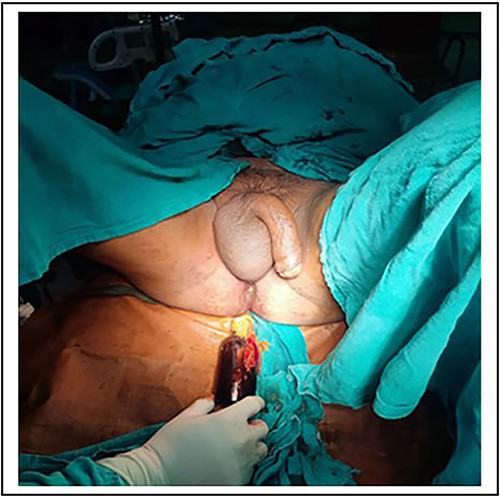
Picture showing removal of foreign body.
DISCUSSION
It was in the 16th century when rectal foreign bodies were first reported [1]. The incidence is said to be most common in Eastern Europe while less common in Asian countries [2]. RFB cases are now frequent presentation in emergency departments, and their incidence is rising, specifically in urban populations [3]. In our case study, the patient is an elderly male who resides in an urban area and presented after 1 d of inserting the cough syrup. Rectal foreign bodies are more common in males than females with an incidence ratio of about 28:1 [4]. Patients are usually males of age around 44 y involved in such activities [3] Although there are various objects inserted in the rectum, glass bottles (42.2%) are most commonly inserted [5]. Sexual gratification, concealment, as may be the case in body packers, sexual assault and, rarely, accidental causes are usual causes but the most common purpose is autoeroticism due to the increasing use of a different object for anal sex [6, 7]. Rectal foreign body is best known in drug traffickers as the body packer [8] Due to the patient’s fear during the history, as he tends not to report what happened objectively patient assessment becomes difficult [9]. Unusual scenarios such as in cases of perforation by glass objects should be given more attention due to their higher risk of perforation [10]. Generally, an average calculated delay of 1.4 d is seen in patients because of embarrassment and other reasons could be they present only after several unsuccessful attempts to remove the object alone, resulting in a late presentation [11].
An abdominal radiograph should be performed before the digital rectal examination to rule out the presence of sharps or glass objects in the rectum, thus avoiding secondary injuries to the patient and the examiner. The digital rectal examination provides us with the concept of anal tone and the approximate distance of the foreign body from the anal verge [12, 13]. Depending on their location relative to the rectosigmoid junction, the rectal foreign body may be classified as high- or low-lying [4]. There are no standard medical protocols for the management of rectal foreign bodies [14]. In sum, 60–70% of FBs can be successfully removed transanally [5]. The standard technique for the transanal approach involves the combined use of analgesia, sedation and anesthesia with an attempt at manual removal of the foreign body [3]. Transanal approaches are contraindicated in peritonitis secondary to rectal perforation, systemic signs of sepsis, investigations showing free gas under the diaphragm on erect CXR and free fluid in the abdomen [5].
Transanal minimally invasive surgical technique (TAMIS) is a newer approach where a laparoscopic trocar is placed through the anus and rubbed to create a seal. Rectum can then by insufflated and laparoscopic graspers are used to grab the object [15]. A more invasive approach includes laparoscopy and laparotomy, where the object is milked toward the rectum for manual removal [16]. If milking of the object distally into the rectum fails, then a colotomy and removal of the foreign object is needed. This colotomy can be primarily repaired. Frank peritonitis, perforation with extensive fecal contamination and unstable patient are good candidates for diversion [2, 8].
CONCLUSION
Rectal foreign body are commonly seen in elderly males with the purpose of auto-erection though there may be various other contributing factor for insertion. The presentation is usually delayed due to the fact that the patient is fearful and is embarrassed causing the late presentation to hospital. Like in our case, it can be managed with manual removal under adequate analgesia. Rectal foreign body poses a greater mortality and morbidity if there is perforation associated with peritonitis.
CONFLICT OF INTEREST STATEMENT
None declared
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}