





Abstract
A 75-year-old woman with a history of multiple myeloma in remission presented with signs, symptoms and imaging findings consistent with a small bowel obstruction secondary to an intussusception. She underwent operative management, and intraoperative findings were consistent with an intussusception of mid small bowel as the cause of the small bowel obstruction. The offending portion of small bowel was resected, and histopathology confirmed a plasmacytoma deposit in the small bowel at the lead point of the intussusception.
Secondary extramedullary plasmacytomas in the gastrointestinal system are rare but can have significant consequences like small bowel obstruction requiring operative management. We present a rare case that emphasizes the need to be highly suspicious for uncommon sequelae of multiple myeloma like secondary extramedullary plasmacytomas when managing patients with history of multiple myeloma in remission with concerning abdominal symptoms.
INTRODUCTION
Multiple myeloma is a malignancy that involves proliferation of clonal plasma cells that originate from the bone marrow [1]. It accounts for 1% of all malignancies and 10% of all haematological malignancies [1]. Although most of the plasma cell proliferation is restricted to the bone marrow, clonal plasma cells can escape and proliferate outside the bone marrow resulting in secondary extramedullary plasmacytomas [2].
Patients with secondary extramedullary plasmacytoma’s tend to have a poorer prognosis due to the ability of plasma cells to proliferate and survive outside the bone marrow’s microenvironment [2]. Secondary extramedullary plasmacytomas are rare in the gastrointestinal tract [3]. Most of the data regarding them are limited to case reports [3–9]. We report a rare case of a secondary extramedullary plasmacytoma in a patient with a history of multiple myeloma in remission, which caused an intussusception resulting in a small bowel obstruction requiring surgical intervention.
CASE REPORT
An independent 75-year-old woman presented to the emergency department with a 1-day history of crampy abdominal pain, nausea, vomiting and constipation. Her medical history includes multiple myeloma, which has been in remission for 4 years. She has no surgical history. On examination, she was alert but distressed with the pain. She was afebrile, normotensive and saturating well on room air with a regular pulse of 110, suggesting sinus tachycardia. Abdominal examination demonstrated a distended abdomen with tenderness around the umbilicus. There were no obvious hernias, and the rest of the abdominal exam was unremarkable. Her haematological investigations were unremarkable, and she had a lactate of 0.9 mmol/L. A computed tomography (CT) of her abdomen and pelvis with intravenous contrast was performed to investigate the cause of her pain. It demonstrated a partial or intermittent mid small bowel obstruction secondary to an intussusception (Figs 1 and 2).

Axial slice of CT abdomen and pelvis showing an intussusception.

Coronal slice of CT abdomen and pelvis showing an intussusception.
Following the investigations, she was diagnosed with intussusception causing small bowel obstruction in a virgin abdomen and was admitted to the general surgical unit for further management. Initial management included insertion of a nasogastric tube, fluid resuscitation and she was kept nil by mouth. She underwent operative management of the small bowel obstruction caused by intussusception under general anaesthesia. The operative findings included some serous peritoneal fluid and mid small bowel intussusception causing small bowel obstruction (Fig. 3). There was a palpable hard lump at the lead point of the intussusception, and there was no other palpable lumps in the mesentery, small or large bowel. A mini laparotomy was made, and a wedge of small bowel with macroscopically clear margins was resected. The rest of the diagnostic laparoscopy was unremarkable. She had an uneventful postoperative recovery and was discharged day 4 post-operation. Histopathology confirmed a 3.1 cm plasmacytoma deposit in the small bowel.
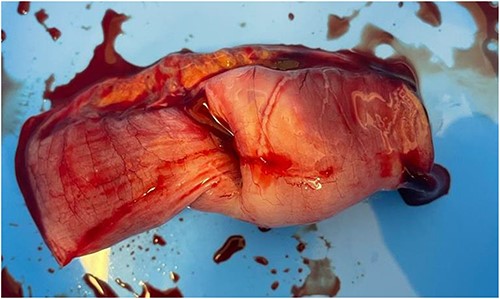
Intraoperative image demonstrating the small bowel intussusception.
She was seen in clinic 3 weeks postoperatively and had no postoperative complications. She was referred to her haematologist for ongoing follow-up and management of her relapsed multiple myeloma.
DISCUSSION
Extramedullary plasmacytomas are malignant plasma clonal cells that migrate and proliferate in soft tissue outside the bone marrow [10]. They make up to 5% of all plasma cell neoplasms [11]. Extramedullary plasmacytomas are divided into two groups: primary and secondary [11]. Primary extramedullary plasmacytomas are solitary tumours that occur in the absence of another plasma cell neoplasm like monoclonal gammopathy of undetermined significance and multiple myeloma [10], whereas secondary extramedullary plasmacytomas are manifestations of another plasma cell neoplasm, commonly multiple myeloma [11].
For this case report, we focused on secondary extramedullary plasmacytomas as that is what our patient had given her history of multiple myeloma. They most commonly occur in that upper aerodigestive tract [10]. Their occurrence in gastrointestinal tract is rare, with an incidence of only 0.9% [12]. Patients with gastrointestinal secondary extramedullary plasmacytomas often present with signs and symptoms that are a consequence of mass effect [3]. They include abdominal pain, bowel obstruction, perforation, melena and haematochezia [3]. In our case, our patient presented with small bowel obstruction because of an intussusception.
A thorough search of the English literature using Google Scholar and Pubmed was conducted, and we found only six other case reports of secondary extramedullary plasmacytomas resulting in small bowel obstruction [4–9]. Like our case, five of these six case reports demonstrate small bowel intussusception as a cause of the obstruction. All six case reports report the incidence of secondary extramedullary plasmacytomas in patients with active multiple myeloma. Our case differs from the rest, as we report the incidence of secondary extramedullary plasmacytomas in a completely well woman who was in remission from her multiple myeloma.
This case emphasizes the need for general surgeons to be vigilant for the malignant causes of small bowel obstructions in virgin abdomens. With increasing survival of patients with multiple myeloma due to improved treatment modalities [3], it is likely that we will see more of the uncommon manifestations of multiple myeloma like gastrointestinal secondary extramedullary plasmacytomas. Previous case reports have demonstrated that secondary extramedullary plasmacytomas in the small bowel only occur in patient with multiple myeloma. We report the first case of secondary extramedullary plasmacytoma in the small bowel causing intussusception in a woman with a history of multiple myeloma that was in remission for 4 years.
In conclusion, a high degree of suspicion for gastrointestinal secondary extramedullary plasmacytomas should be exercised in patients with active or even treated multiple myeloma presenting with concerning abdominal symptoms.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
DATA AVAILABILITY STATEMENT
All data underlying the results are available as part of the article and no additional source data are required.

{kind=link}
{kind=link}
{kind=link}