





Abstract
Congenital pulmonary airway malformation (CPAM) is a developmental malformation that affects the lung parenchyma, especially terminal respiratory bronchioles. This paper reports a case of an infant diagnosed with CPAM who underwent stapleless thoracoscopic lobectomy using Hem-o-Lok clips®. Computed tomography showed cystic pulmonary lesions in the left lower lobe. Thoracoscopic lobectomy was performed at the age of 1 year and 3 months. During surgery, the hilar vasculature was treated using either Hem-o-Lok® clips or a LigaSure vessel sealing system. The lower lobe bronchus was divided using double Hem-o-Lok® clips proximally. The surgery was successfully completed. The patient’s postoperative course was uneventful, and there were no complications. This technique can be easily performed as a thoracoscopic lobectomy with the potential benefits of safe and effective procedures for bronchus closure and vascular sealing in the small working space of pediatric patients.
INTRODUCTION
Congenital pulmonary airway malformation (CPAM) is a congenital disorder of the lung parenchyma characterized by a developmental malformation of the terminal respiratory bronchioles [1]. Thoracoscopic lobectomy is considered the most common minimally invasive surgical approach for CPAM because complete resection of the affected lobe can be achieved [2]. Surgical staplers divide or resect major blood vessels, bronchi and lung parenchyma. However, their application in infants undergoing thoracoscopic surgery remains challenging because of the limited operative thoracic field. Hem-o-Lok® clips (Teleflex Medical, NC, USA) are made from a non-absorbable polymer structure and can be used for several applications in minimally invasive surgery [3].
Herein, we report a case of a simple thoracoscopic lobectomy technique performed on an infant with CPAM using Hem-o-Lok® clips.
CASE REPORT
A male infant with CPAM underwent elective thoracoscopic lobectomy at the age of 15 months; he weighed 9.8 kg. Preoperative computed tomography revealed cystic pulmonary lesions in the left lower lobe (LLL).
Under general anesthesia, one-lung ventilation was used during the surgery. The patient was placed in the right lateral position, and a carbon dioxide pneumothorax was created at an insufflation pressure of 5 mmHg. The 5-mm trocars were placed in the third, fifth, and seventh intercostal spaces in the left midaxillary line. An additional skin incision was placed in the eighth intercostal space on the posterior axillary line. Intraoperative findings showed that the cystic lesion was in the LLL. A complete excision via lobectomy was performed. The left inferior pulmonary vein was identified and taped. An incomplete fissure between the pulmonary segments (S) S4 + 5 and S8 was divided using LigaSure™ (Covidien). After the interlobar pulmonary artery was exposed, the two branches of A6 directly arising from the interlobar portion of the left pulmonary artery, A9 and A10, were divided using LigaSure™ (Fig. 1A). After the pulmonary artery branches A4 + 5 were identified, a medium (M) Hem-o-Lok® clip was applied to the basilar segmental artery A8, which was then sealed and divided distally using LigaSure™ (Fig. 1B). The inferior pulmonary vein was ligated using double Hem-o-Lok® clips (large [L]) proximally and distally, and the vessels were then divided distally using LigaSure™ (Fig. 1C). After confirming the patency of the upper lobe bronchus, the lower lobe bronchus was divided using double Hem-o-Lok® clips (L) proximally (Fig. 1D). An alveolar-pleural fistula with an air leak from the left upper lobe was controlled through intraoperative repair with sutures using fibrin glue and a polyglycolic acid sheet. A chest drain was inserted through the trocar wound. The surgery was successful, with 2 mL of intraoperative bleeding. The patient was discharged on postoperative Day 7.
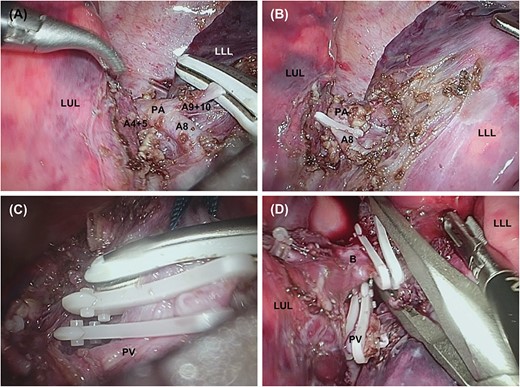
Stapleless thoracoscopic lobectomy procedure. (A) After the PA is exposed, A6, A9 and A10 are sealed and divided with LigaSure™. (B) The Hem-o-Lok® clip is placed on A8 proximally, and the vessel is divided distally with LigaSure™. (C) The left inferior pulmonary vein is double ligated with L-size Hem-o-Lok® clips, then sealed and divided distantly with LigaSure™. (D) Double ligation of the LLL bronchus with L-size Hem-o-Lok® clips and division with scissors. B, left lower lobe bronchus; LUL, left upper lobe; PA, interlobar pulmonary artery; PV, inferior pulmonary vein.
DISCUSSION
The current standard method of thoracoscopic surgery for the hilar vasculature with bronchial closure in pediatric patients includes the use of surgical staplers. Since the introduction of the 5-mm stapler a few years ago, it has been used more frequently for tracheal resection procedures, but its use is quite limited because of complications. Bronchopleural fistula was observed in 5.0% of patients who underwent anatomic pulmonary resection using surgical staplers [4]. The Hem-o-Lok® clip was designed to be retained in the applier jaws to prevent slippage. There are few reports on the use of Hem-o-Lok® clips for bronchial closure in pediatric thoracoscopic lobectomies [5]. This case demonstrates the successful application of Hem-o-Lok® clips for bronchial closure within a limited working space.
Thermal injury is a concern with the use of energy devices, including LigaSure™ [6]. The medium Hem-o-Lok® clip can ligate structures up to 7 mm in size, whereas the large clip can ligate structures up to 13 mm in size, which is adequate to close the lobe bronchus and major vessels in infants. However, instances of slippage and clip migration into the surrounding viscera have been reported in pediatric patients and should be considered prior to surgery [7, 8]. In experimental animal models, the Hem-o-Lok® clip failed at bursting pressures, when compared with a mechanical stapler, and had the worst holding strength of all the various clips used when applied to the pulmonary vessels, because they have thinner layers [9, 10]. Hence, the authors suggested that leaving some tissue around the vessels may increase their thickness, which may increase the holding strength. In the present case, LigaSure™ was used to divide the vessels after the clips were applied, and the seal was maintained if the Hem-o-Lok® clips slipped. Furthermore, some experience is required before using mechanical staplers because of the limited thoracic cavity, especially in infants with CPAM. In contrast, the Hem-o-Lok® clip is accessible to surgeons with no prior experience. Additionally, a rapid and secure alternative to intracorporeal sealing techniques in infants undergoing thoracoscopic lobectomy might decrease anesthesia and surgical duration. Moreover, another advantage of Hem-o-Lok® clips is the reduced cost compared with mechanical staplers [11].
CONCLUSION
This technique can be easily performed for a thoracoscopic lobectomy and has the potential benefits of being a safe and effective procedure for bronchial closure and vascular sealing in infants.
ACKNOWLEDGEMENTS
We would like to thank Editage (www.editage.com) for English language editing.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
All authors declare that they have no conflict of interest.
AUTHORS’ CONTRIBUTIONS
K.M. drafted the manuscript. K.M., N.U., M.N., M.K. and H.O. performed the surgeries and critically revised the manuscript. All authors read and approved the final manuscript.
DATA AVAILABILITY
The data sets analyzed during the current study are available from the corresponding author on reasonable request.
CONSENT FOR PUBLICATION
Informed consent was obtained from the patients for publication of this case report.

{kind=link}