





Abstract
Mesenteric fibromatosis is a rare tumor that grows slowly and asymptomatically and is more frequent among men. The risk factors described in the literature may not be present in all cases. The clinical presentation is variable and depends on the localization of the tumor and the involvement of surrounding structures. Imaging studies such as abdominal computed tomography and magnetic resonance imaging are the preferred methods for the diagnosis of this tumor. However, a definitive diagnosis is made based on histopathology and immunohistochemistry results. Surgical resection remains the preferred option for the treatment of mesenteric fibromatosis. This report presents a clinical case of mesenteric fibromatosis in a male patient who presented with partial abdominal obstruction and the absence of risk factors for mesenteric fibromatosis.
INTRODUCTION
Mesenteric fibromatoses are monoclonal, myofibroblastic, neoplastic proliferations that tend to show a locally aggressive behavior. They are classified into superficial and deep tumors, and the deep type is known as a desmoid tumor [1, 2]. Desmoid tumors, which are the most common primary tumors of the mesentery, were first described in 1832 [2–5]. They are rare tumors, accounting for 0.03% of all neoplasms and 3.5% of all fibrous tissue neoplasms [4, 6].
Desmoid fibroma is a soft tissue tumor that is histologically benign but locally aggressive; it originates from the fascia or muscular aponeurotic structures and shows a tendency to invade adjacent tissues [5, 6]. Desmoid tumors are classified as extra-abdominal and abdominal. They show variable localization, and the abdominal form is more frequent (57%) than the extra-abdominal form (43%) [3, 7].
Abdominal desmoid tumors include several entities that show similar morphological features but different clinical presentations [1, 8, 9]. According to their localization, they can vary from an asymptomatic mass to a clinical presentation of intestinal obstruction and hydronephrosis, bleeding or perforation of a hollow organ [3].
The objective of this report is to present a case of mesenteric fibromatosis in a male patient with a clinical picture of a partial abdominal obstruction.
CLINICAL CASE PRESENTATION
A 43-year-old man underwent exploratory laparotomy for acute appendicitis 11 months prior to this presentation in which a mesenteric mass was detected perioperatively. The patient presented to our center with a 24-h history of colicky, diffuse abdominal pain without an apparent cause that was of moderate intensity and accompanied by nausea and vomiting on various occasions. Physical examination revealed a complaining patient with a distended abdomen that was painful on palpation at the right hypochondriac region and right iliac fossa. A fixed mass measuring 10 cm in diameter was palpated in the right inferior quadrant and bowel sounds were increased. Biometric screening results and the urea creatinine ratio were normal. Tumor markers including CA 19–9, alpha-fetoprotein and carcinoembryonic antigen levels were within the normal range. Abdominal computed tomography with and without contrast showed a solid intra-abdominal mas at the right paraumbilical level measuring 70 mm in the largest diameter and adjacent to the right colon. The mass was round and had a regular, well-defined contour with signs of central necrosis, compressing the distal segment of the small intestine (Fig. 1). Colonoscopy was normal.
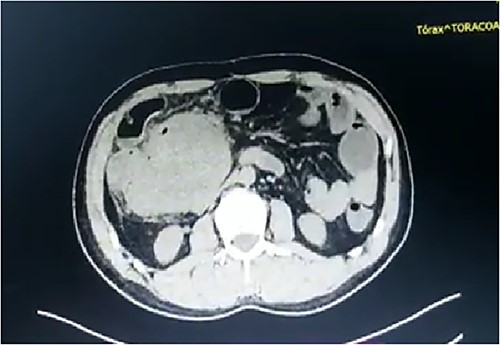
Abdominal computed tomography showing an intra-abdominal mass measuring 70 mm in diameter and compressing the small intestine.
The patient underwent an emergency laparotomy. The findings were a retroperitoneal heterogeneous mass with a hard consistency measuring ⁓10 × 10 cm invading the third portion of the duodenum, 40 cm of the terminal ileum, cecum, ascending colon and part of the transverse colon with the presence of lymph nodes in the mesentery. A resection of the retroperitoneal mass and right hemicolectomy were performed, as well as end-to-end ileocolonic anastomosis and suture of the duodenum due to incidental perforation with drain placement (Fig. 2A and B). Postoperatively, the patient showed adequate evolution, starting an early diet with adequate tolerance and intestinal transit. The patient was discharged in good condition.
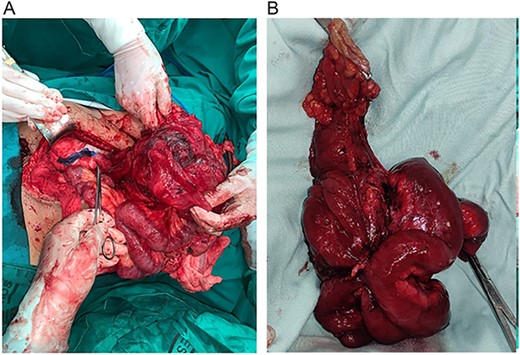
(A) Retroperitoneal mass invading the right colon, terminal ileum and part of the transverse colon. (B) Resected tumor sample for histopathology.
Histopathology showed a tumoral mass measuring 10 × 9 × 9 cm at the distal end of the mesenteric side of the ileum. Macroscopically, the lesion reached the submucosal layer. Microscopically, the sections showed a lesion consisting of a proliferation of fusiform cells with large and hyperchromatic nuclei intercalated with intervening collagenized material (Fig. 3). The lesion extended to the ileum, where the mucosa was eroded. Immunohistochemistry was negative for CD34, CD57 and ALK-1, whereas the fusiform cells were positive for actin, CD99 and β-catenin. Based on previous results, a diagnosis of mesenteric fibromatosis was made.
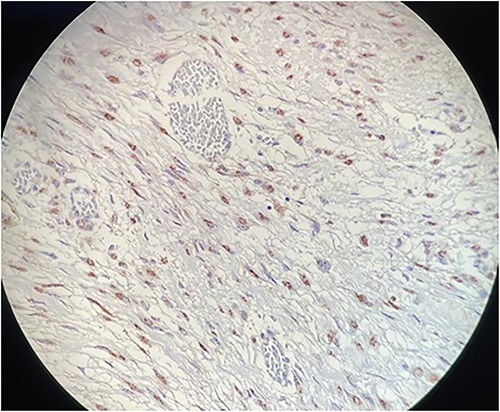
Microscopy: fusiform cell proliferation with positive β-catenin immunoreactivity.
DISCUSSION
Mesenteric fibromatosis is a rare neoplasm of myofibroblastic origin that does not metastasize but is locally aggressive and frequently presents with recurrences [6, 7]. It can have various presentations, and it most commonly presents as part of a familiar adenomatous polyposis or Gardener syndrome; in some cases it is associated with Crohn’s disease. It can present as a sporadic case with lower frequency [6, 10].
The tumor appears most frequently in the mesentery of the small intestine, as in the present case, whereas it is less frequently localized in the transverse mesocolon, gastro-hepatic ligament and gastro-splenic ligament [7, 9].
These tumors present as insidious and asymptomatic masses that invade adjacent structures and are found incidentally during a physical examination [3, 7]. According to their relation to adjacent organs, they can cause severe complications, such as intestinal obstruction, perforation, ischemia, hydronephrosis, fistula and even aortic rupture or infiltration of the hepatic portal tracts with obstructive jaundice [7]. The present case presented with the clinical picture of a partial intestinal obstruction [1].
The risk of mesenteric fibromatosis increases in association with previous surgery, trauma, estrogen and pregnancy. The onset age varies from 8 to 72 years with an average age of ⁓46.2 years [3, 4, 7]. It is more common in women than in men.
Among imaging studies, magnetic resonance and computed tomography are effective modalities for the diagnosis of mesenteric fibromatosis [2]. However, lesions that involve the stomach or intestine may appear to originate in these sites and simulate a different pathology such as a primary gastrointestinal tumor [7, 9]. For the differential diagnosis of Gardner syndrome or adenomatous polyposis, a colonoscopy is recommended. Histopathology and immunohistochemistry are useful for making a definitive diagnosis. The macroscopic appearance of the desmoid tumor is a pale surface with scant vascularization [7]. Microscopically, fusiform cells rich in acidophilic cytoplasm are observed (9,12). Immunohistochemically, mesenteric fibromatosis can be positive for actin and less frequently for desmin, whereas it is usually positive for nuclear β-catenin expression and negative for CD34 immunostaining [1].
In the majority of cases, the treatment is surgical. Recurrent mesenteric fibromatosis can also be resected, although this is associated with increased morbidity and mortality [7]. Radiotherapy is a treatment option for advanced or recurrent mesenteric fibromatosis [3, 4, 11].
The present case was a patient who had been followed-up for an abdominal mass detected in a previous laparotomy. A computed tomography performed prior to this admission suggested findings consistent with Castleman disease. However, resection of the mass and histopathology confirmed a diagnosis of mesenteric fibromatosis.
In conclusion, mesenteric fibromatosis is a rare tumor that generally grows at a slow rate and is asymptomatic. There are several risk factors that may not be present in all cases. Computed tomography and magnetic resonance imaging are the preferred methods for the diagnosis of this condition. However, histopathology and immunohistochemistry are necessary for a definitive diagnosis. Surgical resection is the treatment of choice for mesenteric fibromatosis.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}