





Abstract
Six years prior, the patient accidentally swallowed a denture during a meal and immediately visited a nearby doctor. However, because spontaneous excretion was expected, regular imaging testing was used to monitor it. After 4 years, although the denture was still in the small bowel, as there were no symptoms, the regular follow-up was terminated. Because the patient’s anxiety increased, he visited our hospital 2 years later. Surgery was performed, as it was determined that there was no possibility of spontaneous excretion. The denture was palpated in the jejunum. The small intestine was incised, and the denture was removed. As far as we know, there are no guidelines prescribing a clear follow-up period for accidental denture ingestion. In addition, there are no guidelines specifying surgical indications in asymptomatic cases. Nonetheless, there have been reports of gastrointestinal perforations with dentures, and we consider that earlier preventive surgical intervention is better.
INTRODUCTION
Making and using dentures for toothless cases are indispensable for daily life. As the aging society increases, the number of people who use dentures will continue to increase. Accidental ingestion and aspiration of detachable dentures are sometimes encountered in medical practice.
Gastrointestinal foreign bodies are expected to be excreted spontaneously. It has been reported that ~20% of cases require endoscopic removal, and ~1% require surgical procedures. Furthermore, it has been reported that the absolute indication for surgery is in cases of gastrointestinal perforation, and the relative indication is incomplete endoscopic treatment [1]. The indications for endoscopic removal of gastrointestinal foreign bodies are described in detail in the European Society of Gastrointestinal Endoscopy (ESGE). However, the indications are limited to the range that can be reached by upper gastrointestinal endoscopy, and unfortunately, descriptions of how to handle foreign matter that has flowed to the anal side of the duodenum are not mentioned [2].
CASE REPORT
A 73-year-old male visited our hospital without symptoms. He claimed that he accidentally swallowed a denture 6 years before, and it still remained in his gastrointestinal tract. Although there were no symptoms, he was anxious and wanted it to be removed.
Six years ago, he accidentally swallowed the denture during a meal and immediately visited the nearby hospital. Although the swallowed denture was observed in the stomach by X-ray examination, there was a large amount of residue in the stomach, as it was after a meal. The doctor judged that emergency upper gastrointestinal endoscopy was dangerous and decided to perform it the next day. The next day, before endoscopy, X-ray was reexamined, and it was found that the denture had already flowed out from the stomach and reached the duodenum. Since it had flowed into the duodenum, the doctor determined that spontaneous excretion could be expected, and he decided to follow up by regular imaging examination. Since then, computed tomography (CT) and X-ray examinations have been performed regularly. Although the denture remained in the small intestine, as there were no symptoms, follow-up was continued for 4 years. After 4 years, the patient was told to visit when any symptoms appeared, and regular follow-up was terminated by the doctor.
Abdominal examination findings were normal. Blood exams showed no unusual findings except slight renal dysfunction (BUN 38.2 mg/dl, Cre 1.98 mg/dl). We asked the previous doctor to provide the results of the imaging test (Fig. 1a and b). After that, we performed X-ray (Fig. 2a) and CT (Fig. 2b) examinations at our hospital and confirmed that the denture was still in the small intestine. Since it remained in the intestinal tract for a long time, there was no possibility of spontaneous excretion. Although the patient was asymptomatic, we decided to perform surgery because the patient himself wanted to have it removed.
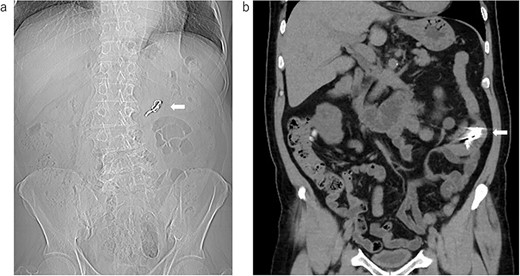
The image data were obtained by the previous doctor; (a) X-ray examination: the arrow shows the swallowed denture; (b) the coronal image of the CT: the arrow shows the swallowed denture.
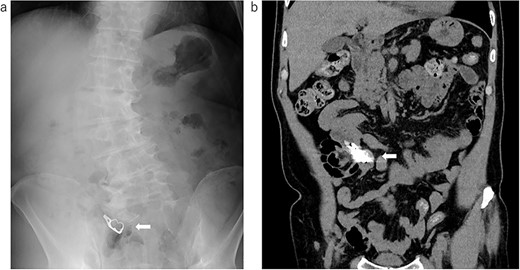
The image data were obtained at our hospital; (a) X-ray examination: the arrow shows the swallowed denture; (b) the coronal image of the CT: the arrow shows the swallowed denture.
Under general anesthesia, the abdomen was opened with a small incision of 5 cm in the mid-abdomen. There were no ascites or adhesions. The foreign body was palpated in the jejunum, 60 cm from the ligament of Treitz. There were no abnormal findings on the serosal surface (Fig. 3a). An incision was made in the small intestine, and the foreign body was tried to remove. However, the hook part was tightly involved with the mucosal membrane and could not be removed (Fig. 3b). Therefore, when we tried to bend the hook portion with forceps, the hook portion was damaged, and as a result, extraction became possible (Fig. 3c). After confirming that there was no damage to be repaired on the mucosal surface and that no foreign matter had fallen into the abdominal cavity, the incised small intestine was closed with sutures.
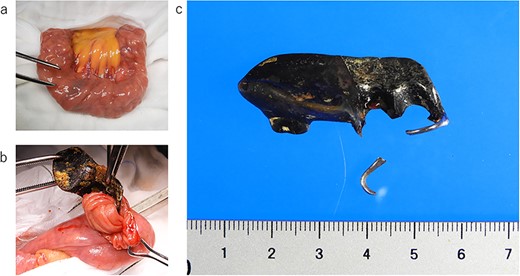
Intraoperative photograph and image of the removed denture; (a) the small intestine removed outside the body: there were no abnormal findings on the serosal surface; (b) a denture found in the small intestine: the hook part involved the small intestinal mucosa; (c) removed denture: the hook part is damaged during extraction.
DISCUSSION
In this case, the hooked denture, which could perforate the gastrointestinal tract, reached the small intestine, but nothing happened for a long period. Since there were no abnormal findings on the serosal surface, it can be said that the judgment of the previous doctor who continued to monitor the progress was correct. However, this situation will not fit all cases. The point to be discussed in this case is whether preventive surgical excision should be performed when a foreign body in the gastrointestinal tract has flowed to an area that is inaccessible by the endoscope. Another point is the follow-up period for gastrointestinal foreign bodies with sharp points at risk of gastrointestinal perforation.
It is tempting to assume that dentures with hooks are more likely to damage the gastrointestinal tract, but there were two reports that showed no statistical relationship between denture shape and the risk of perforation or penetration [3, 4]. The duration from accidental denture ingestion to perforation or penetration of the lower gastrointestinal tract ranges from 1 day to 6 months [5, 6]. Considering these references, regardless of the shape of the denture, there is a risk of gastrointestinal perforation or penetration if dentures are accidentally swallowed and reach the lower gastrointestinal tract. Spontaneous excretion is expected if the swallowed denture passes through the duodenum, but there is a possibility that perforation or penetration may occur at any time during 6 months. In other words, the life-threatening period is the first 6 months after accidental ingestion of dentures. However, living for half a year with the possibility of perforation at any time is considered to be a great stress for the patient. Although it is unclear whether these data are taken into consideration, other reports suggest that surgery should be considered if the ingested foreign body that has flowed into the lower gastrointestinal tract remains in the same site for 1 week [1].
Regarding denture ingestion, there is a risk of gastrointestinal perforation or penetration regardless of the shape of the denture, which can occur within 1 day. Therefore, in the early stages of accidental ingestion of dentures, follow-up observation during hospitalization is considered preferable. Although it depends on the patient’s general condition, even if the patient is asymptomatic, surgery should be considered if the accidentally swallowed denture remains in the same site for 1 week.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
INFORMED CONSENT
The patient’s consent for publication was obtained in writing.

{kind=link}
{kind=link}
{kind=link}