





Abstract
Treatment options for distal femur fractures include open reduction internal fixation (ORIF), arthroplasty, or a hybrid of both. We present a 76 year old female with left knee pain secondary to known osteoarthritis, known lateral condyle insufficiency fracture, and an acute medial condyle fracture. In order to solve the acute and chronic problems in a single procedure, a combined ORIF and constrained condylar knee (CCK) arthroplasty was performed. Arthroplasty alone would have required a highly constrained distal femur replacement, and ORIF alone would have caused prolonged immobilization and continued morbidity from unaddressed chronic problems. We chose a CCK as a less constrained implant would not have protected our ORIF which contained the medial collateral ligament attachment. This technique avoids the complications of ORIF alone, and avoids the known complications of increased constraint in total knee arthroplasty.
Introduction
Distal femur fractures are traumatic injuries that happen across all age groups. Management includes non-operative intervention for minimally displaced fractures or patients too ill to undergo intervention. Operative management can range from open reduction internal fixation (ORIF), arthroplasty, or a combination of both. The decision becomes more challenging when dealing with atypical fracture patterns, concurrent osteoarthritis, or need for early weight bearing. Treating distal femur fractures with ORIF or arthroplasty is well documented. Rare in the literature has it been proposed to use a combination of both. Here we present a case of an elderly female suffering from known tri-compartmental osteoarthritis and lateral condyle insufficiency fracture. Subsequently the patient presented with an acute fracture of the medial femoral condyle. Management consisted of medial condyle ORIF and constrained condylar knee (CCK) arthroplasty to prevent the risk of ongoing morbidity to the patient if either intervention were performed alone. We present this case report along with the review of literature to provide the orthopedic community with an alternative management strategy if faced with a similar scenario.
Case report
We present the case of a 76 year old Hispanic female previously managed for tri-compartmental osteoarthritis and lateral condyle insufficiency fracture of the left knee. She was being managed conservatively; however, the pain began to affect her well-being and activities of daily living (ADL). Most recently the patient suffered a mechanical ground level fall resulting in an ipsi-lateral medial condyle fracture as seen in Fig. 1. Single staged left knee medial condyle ORIF and CCK arthroplasty through a medial para-patellar approach was performed. The medial condyle fracture was reduced and stabilized using a 5-hole distal fibula locking plate in buttress mode. After fracture stabilization, a CCK arthroplasty was performed. Immediate post-operative imaging is seen in Fig. 2. Intra-operative photos are demonstrated in Fig. 3. The patient was made non-weight bearing for 2 weeks followed by weight bearing as tolerated (WBAT). An early weight bearing protocol was used given the majority of forces during ambulation would be placed through the total knee implant and not place significant stress on the medial condyle ORIF. At 3 months post-operatively, the patient obtained 0–120° range of motion (ROM) and was freely WBAT. At 8 weeks, however, the patient required a manipulation under anesthesia for regressing to 0–95° ROM. Figure 4 demonstrates intra-operative images of the manipulation. At 3 years follow up, her ROM was 5–95 with good strength without any further complication or subsequent procedures. Three years post-operatively the patient reported improved function with ADLs, significantly improved pain, and better mental health.
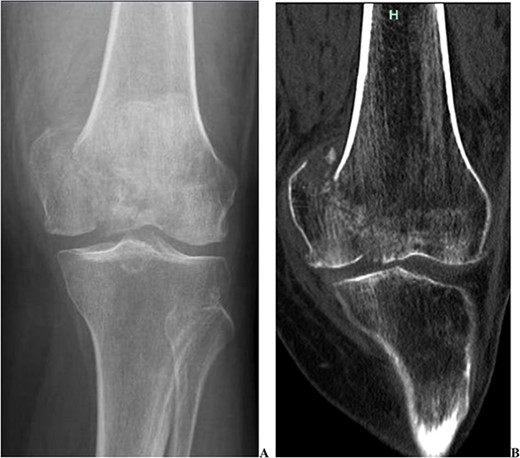
Two pre-operative injury images demonstrating the acute medial condyle distal femur fracture of the left knee. In addition to the acute fracture, one can appreciate the pre-existing osteoarthritis. (A) Radiograph demonstrating a large displaced medial condyle fracture. (B) CT scan re-demonstrating the acute medial condyle fractures.

Two post-operative radiographs of the left knee demonstrating the constrained condylar knee arthroplasty, along with the open reduction internal fixation of the medial condyle using a distal fibula locking plate in buttress mode.
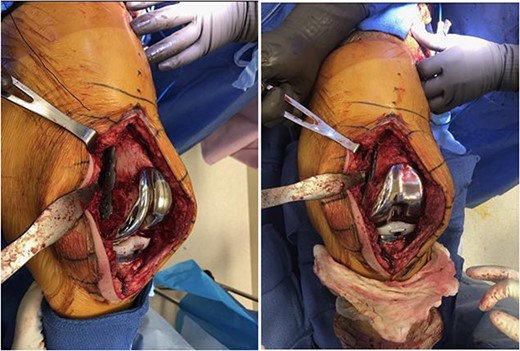
Two intra-operative images demonstrating the medial para-patellar approach used the open reduction internal fixation of the medial condyle with a distal fibula locking plate, and the constrained condylar knee arthroplasty. These images demonstrate the final construct immediately prior to closure.
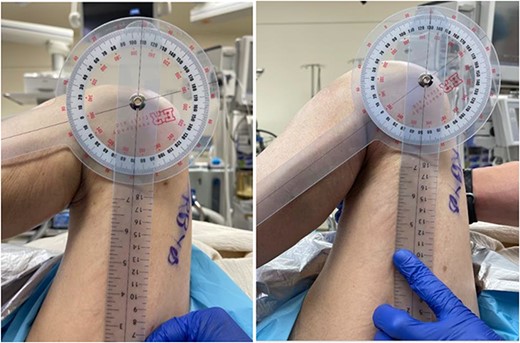
Two intra-operative images demonstrating the pre-manipulation flexion of 70°, and the post-manipulation flexion of 115°.
Discussion
When it comes to ORIF of distal femur fractures, the goal is to restore the native anatomy and provide an ideal environment for fracture healing. In the elderly, an additional goal is for early weight bearing as post-operative immobility contributes to increased complications and rapid decline in health [1]. Open reduction internal fixation of the distal femur generally includes plate and screw constructs or intramedullary nailing (IMN). Intramedullary nailing provides enough stability to facilitate early weight bearing, and has the added benefit of preserving soft tissue biology [2]. Additionally, IMN has historically been used for extra-articular fractures, although successful management with articular involvement has been discussed in the literature [2]. On the other hand, ORIF with plate and screw constructs has historically been used when there is articular involvement. This is largely to achieve anatomic reconstruction of the articular surface to preserve the native joint [3]. In this case we elected to use a plate and screw construct given the articular involvement, and because the displaced fragment included the MCL attachment which required anatomic reduction. Additionally, the CCK implant would not work with an IMN in place.
Arthroplasty is another valid treatment for distal femur fractures in the elderly. Immediate arthroplasty has many benefits including eliminating fracture healing issues and early weight bearing [4]. This management strategy can be beneficial in patients with poor bone quality, pre-existing degenerative joint disease, and medical problems [4]. Many elderly patients have some level of underlying cartilage degeneration requiring arthroplasty after fracture healing in primary ORIF [4]. Treating with arthroplasty initially eliminates the complications associated with a delayed arthroplasty. Delayed arthroplasty is often complicated by distorted anatomy, joint contractures, and the unpredictability of hardware removal [4]. Thus, initially treating distal femur fractures in patients with pre-existing arthritis is beneficial. Additionally, recent literature suggests relatively low revision rates and good implant survival rate at long term follow up when knee arthroplasty is performed for fractures in the native knee [5].
Our patient’s most urgent problem was the acute medial condyle fracture. Treating this problem with ORIF alone would have required prolonged immobilization, restricted ROM given the MCL attachment, and included the unpredictability of fracture healing. Additionally the articular surface of the medial condyle was much more comminuted than pre-operative imaging demonstrated, causing a very unstable and unsupportive articular surface. Moreover, ORIF alone would not have addressed her other two problems including debilitating end stage osteoarthritis and lateral condyle insufficiency fracture. The other option would have been to treat this with arthroplasty alone. Given the extent of the medial condyle involvement this would have required a highly constrained implant such as a distal femur replacement (DFR). As we will discuss this carries the complication and risks associated with increasing constraint in total knee arthroplasty.
Increasing constraint in knee arthroplasty offers more stability to the implant, but does so at the cost of causing increased forces being transmitted to implant interfaces and potential subsequent aseptic loosening [6]. From least to most constrained you generally have cruciate retaining, posterior stabilized, CCK, hinged, and DFR implants [7]. With increasing constraint there are significant items to consider regarding ROM and functional capacity, which become limited with higher constraint [8]. Greater constraint can cause increased and uneven stress distribution within the joint, potentially leading to problems like stress shielding, aseptic loosening, and ultimately implant failure [7]. Therefore, the immediate stability achieved with increased knee constraint must be weighed against the long term complications and functional limitations. Our choice to use a semi-constrained implant was driven by the need to protect our ORIF, which included the MCL attachment. Any less constraint would have put a lot of stress on the MCL attachment and plate and screw construct.
By implementing a hybrid of two techniques, we aimed to mitigate potential complications and morbidity associated with ORIF or arthroplasty alone. This patient centered approach seeks to strike a balance between immediate fracture stability and preservation of joint function. We believe that this combination presents an effective alternative management approach when dealing with similar clinical scenarios, ultimately striving to optimize patient outcomes.
Conflict of interest statement
None declared.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Consent
Written and verbal consent were obtained from the patient for publication of this case, clinical findings, and related images. Written consent is available to the Editor-In-Chief upon request.

{kind=link}
{kind=link}
{kind=link}
{kind=link}