





Abstract
Spinal arachnoid webs are intradural bands of abnormally formed arachnoid tissue, located within the subarachnoid space and causing compression of the dorsal aspect of the spinal cord. Arachnoid webs are uncommon and can be difficult to treat. We report 3 patients presenting with a spinal arachnoid web within a 6-month period. All of them exhibited signs of thoracic myelopathy and the MRI showed the pathognomonic ‘scalpel sign’. Two of the patients underwent surgery for removal of their spinal arachnoid web, whereas the third patient case is currently being managed conservatively. We also present our 2D intraoperative video for arachnoid web removal and spinal cord decompression.
Introduction
Spinal arachnoid webs are thickened intradural bands of arachnoid tissue that can extend to the pial surface of the spinal cord [1]. These spinal webs are rare entities that can cause mass effect and a dorsal indentation of the spinal cord. Typically, spinal arachnoid webs occur in the upper thoracic spine and may produce the pathognomonic radiographic ‘scalpel sign’ [2]. This scalpel sign can be seen on sagittal MR imaging and is due to the arachnoid web causing a dorsal indentation of the upper thoracic spinal cord. When left untreated spinal arachnoid webs can result in a range of neurological dysfunctions, typically causing progressive myelopathy in otherwise healthy individuals [3]. The arachnoid webs are occasionally associated with syringomyelia [4].
The investigation and diagnosis of patients with spinal arachnoid webs can be extensive, requiring multiple studies to confirm the diagnosis. Currently, the gold standard for radiological diagnosis is magnetic resonance imaging (MRI), but the thin size of certain arachnoid webs can result in suboptimal sensitivity [5]. Furthermore, the use of computed tomography myelogram can miss the presence of spinal arachnoid webs, as they typically do not cause complete cerebrospinal fluid (CSF) obstruction. Since conventional studies can miss the diagnosis, the use of MRI with constructive interference with steady state can also be used to properly identify and visualize the webs [6]. Intraoperative diagnostic studies also play a key role in locating and properly treating arachnoid webs. During surgical exploration, following the initial laminectomy, an intraoperative ultrasound can be used to locate the arachnoid web prior to the dural opening [7, 8].
This report is a retrospective case review of 3 patients presenting with a spinal arachnoid web within a 6-month period. The age range was 40–67 years of age, with 1 male and 2 females. The 3 patients presented with a range of neurological symptoms, including thoraco-lumbar pain, myelopathy, and thoracic radiculopathy. All 3 patients demonstrated a characteristic scalpel-shaped deformity on imaging. Two of the patients underwent surgery for removal of their spinal arachnoid web, which included a thoracic laminectomy with spinal cord release. The two cases of surgical intervention and their outcomes are described below. One case is currently being managed nonoperatively.
Case reports
Patient A
A 67-year-old man presented with a 1-year history of midline back pain that radiated down his right side and myelopathic symptoms. He stated that his symptoms worsened over the last year, and he felt generally weak in the lower extremities, causing problems with ambulation. He did not have any bowel or bladder incontinence, and there was no history of spinal surgery or syrinx expansion. MR imaging demonstrated a spinal cord indentation along the dorsal surface of the spinal cord at the T5 vertebral body level (Fig. 1a). It was hypothesized that the appearance of the spinal cord indentation was secondary to an arachnoid web. The patient underwent T5-T6 laminectomies for intradural exploration for arachnoid web resection at the level of the spinal cord narrowing. The arachnoid web was inspected, and the area of tether was identified and removed using microsurgical tools and technique (Video S1). Postoperatively, the patient reported improvement in back pain, increased strength within the lower extremities, and mild chest wall numbness. Follow-up MR imaging demonstrated resolution of the dorsal indentation and cord expansion (Fig. 1b).

(a) Dorsal indentation (scalpel sign) demonstrated in thoracic spine preoperatively (Patient A). (b) Postlaminectomy and resection of posterior arachnoid web demonstrating resolution of dorsal indentation and cord signal changes (Patient A).
Patient B
A 40-year-old woman presented with a 3-year history of progressively worsening interscapular pain radiating around the rib cage on the right, difficulty with ambulation, and right foot numbness. Physical examination demonstrated myelopathic symptoms, with 3+ reflexes in both lower extremities, clonus, and Babinski, as well as difficult tandem gait. Thoracic MRI showed an arachnoid web at the T5-T6 vertebral levels (Fig. 2a). The patient underwent a T5-T6 laminectomy with intradural exploration. A large arachnoid web was encountered and resected using microsurgical tools and technique. Postoperatively, the patient reported improvement in her pain and ambulation. Follow-up MR imaging demonstrated resolution of the dorsal indentation and cord expansion (Fig. 2b).

(a) Dorsal indentation demonstrated in thoracic spine preoperatively (Patient B). (b) Postlaminectomy and resection of posterior arachnoid web demonstrating resolution of dorsal indentation and cord signal changes (Patient B).
Patient C
A 62-year-old woman presented with an extensive, multi-decade history of lower back pain that has progressively gotten worse over the last year. She initially presented in clinic with lumbar pain that radiated down her left anterior thigh, as well as significant thoracic pain that worsened with activities. She has a past surgical history of three lumbar laminectomies in 1983, 1988, and 1995 that caused temporary relief of her lumbar radiculopathy. In clinic, she stated that, during long periods of standing, she will experience buttock and lower extremity pain, as well as pain radiating to her anterior thigh and groin. She also said that she had increased difficulty with balance, causing her to use a rolling walker for ambulation. Physical examination demonstrated myelopathic symptoms with 3+ reflexes in both lower extremities and positive Babinski sign bilaterally. MR imaging of the spine was ordered and showed an arachnoid web displacing the spinal cord at the level of T3 (Fig. 3). Her current symptoms were treated nonoperatively with an epidural steroid injection that caused 80% relief of symptoms for 2–3 weeks. Three months later, she returned with increased bilateral shooting pain in the interscapular blade region. The patient will return in 6 months to proceed with a repeat thoracic MRI to evaluate for any interval changes.
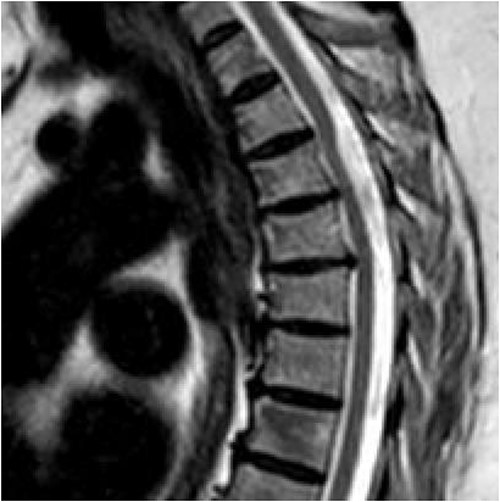
Dorsal indentation demonstrated in thoracic spine preoperatively (Patient C).
Discussion
Spinal arachnoid webs represent a rare clinical condition caused by an uncertain etiology, primarily manifesting in the dorsal region of the thoracic spine [1]. Despite their infrequency in medical literature, these arachnoid webs exert a profound impact on patients' quality of life, often leading to pronounced myelopathic symptoms and neurological deficits. Among the three cases explored in our study, two received surgical management, reporting notable postoperative improvements.
The favorable postoperative outcomes observed in our initial two patients underscore the potential effectiveness of surgical intervention as a curative therapeutic option. Specifically, surgical excision and lysis of the spinal arachnoid web offer a compelling strategy for mitigating neurological deficits associated with symptomatic spinal cord compression. This is exemplified in the case of Patient C, whose conservative management failed to provide sustained symptom relief and will likely require surgical intervention in the near future.
Several studies have delved into the efficacy of surgical interventions for patients diagnosed with spinal arachnoid webs, yielding valuable insights into treatment outcomes [3, 5, 9, 10]. Notably, Nisson et al. [10] conducted an extensive investigation, reporting a noteworthy 91% rate of neurological improvement among patients subjected to surgery as part of their treatment regimen. Additionally, Hirai et al. [11] demonstrated partial neurological improvement in five cases within their study cohort. These collective findings underscore the potential advantages of surgical intervention as a viable therapeutic approach for individuals grappling with spinal arachnoid webs.
In a three patient case series authored by Yamaguchi et al., the emphasis is placed on surgical lysis and complete removal of the thickened arachnoid web as the preferred treatment strategy. This approach not only rectifies spinal cord compression but also addresses any CSF blockage [12]. The improvement after surgical decompression has been shown to be long-lasting [13]. A meta-analysis by Ben Ali et al. [5] suggests an individualized treatment approach, driven by the diverse array of neurological deficits associated with spinal arachnoid webs. They advocate that patients presenting with symptomatic cord compression and CSF blockage should undergo surgical lysis and removal, while those manifesting variable neurological deficits without CSF blockage may initially derive benefit from conservative management before considering surgical intervention [5]. Other authors have compared the outcomes of patients undergoing surgical decompression versus conservative treatment and found that nonoperative patients did not improve [14].
In conclusion, our findings contribute to a more comprehensive understanding of treatment options for patients with spinal arachnoid webs, emphasizing the potential benefits of tailored surgical approaches and the importance of considering individual patient profiles in clinical decision-making. Going forward, it is advisable that patients diagnosed with spinal arachnoid webs receive surgical intervention if they exhibit symptomatic cord compression and partial CSF flow obstruction. While conservative management may be suitable for select cases, it is crucial to recognize that arachnoid webs do not self-resolve, necessitating surgical excision and lysis for sustained symptom relief throughout a patient’s lifetime. These studies not only underscore the overall positive impact of surgical management on neurological outcomes but also highlight the need for further exploration and research in this domain. Such insights are critical for advancing our understanding of spinal arachnoid web treatment strategies and ultimately enhancing the quality of care provided to affected patients.
Conclusion
Effectively managing patients with spinal arachnoid webs presents a multifaceted challenge. The critical first step is the timely radiological recognition of the pathognomonic scalpel sign. Failing to diagnose and treat arachnoid web cases accurately can lead to a deterioration of neurological function, with subsequent improvement often requiring surgical intervention. As highlighted by the surgical cases discussed earlier, the removal of the arachnoid web has consistently demonstrated substantial symptom relief. In contrast, conventional laminectomies, which do not address the web itself, have proven ineffective in providing relief to afflicted patients. These observations underscore the pivotal role of precise diagnosis and surgical intervention in the management of spinal arachnoid webs, advocating for a more tailored and effective approach to enhance patient outcomes.
Conflict of interest statement
None declared.
Funding
No funding was received for this article.

{kind=link}
{kind=link}
{kind=link}