





Abstract
Coeliac disease, a relatively rare gluten-sensitive enteropathy, correlates with small intestinal malignancies, especially lymphoma and adenocarcinoma. Any kind of masses, whether malignant or benign, in the way of natural peristaltic action may increase the probability of intussusception, telescoping invagination of the proximal segment into the distal one causing an obstruction. We report a case of synchronous adenocarcinomas of the colon and jejunum in a 3-year-old female presenting as bowel obstruction. She also had coeliac disease. During laparotomy, the surgical team encountered jejunojejunal intussusception as the cause of obstruction. There are direct relationships among coeliac disease, increased risk of adenocarcinoma, and repeated intussusceptions in the absence of mass in adults. The intussusception phenomenon in an adult necessitates investigating a more severe lead point than simple mesenteric lymphadenopathy.
Introduction
The correlation between celiac disease, an enteropathy induced by ingesting gluten-containing foods, and malignancies has already been proved. Among them, non-Hodgkin lymphomas and gastrointestinal tumours are the most typical neoplasms associated with celiac. The associations with enteropathy-associated T-cell lymphoma and small bowel adenocarcinoma are well understood [1, 2]. Intussusception is defined as a condition in which a proximal segment of the intestine invaginates into the neighbour segment in a telescoping style. Typically, intussusception is observed in a child with a recent upper respiratory infection, causing mesenteric lymph nodes to enlarge. These lymphadenopathies act as lead point barriers inducing the invagination event. Since intussusception as a cause of bowel obstruction is rare in adults, the physician should investigate malignant tumours as lead points. Having reported a case of synchronous adenocarcinomas of small and large intestines in a 33-year-old female with celiac disease who underwent resolution for obstruction and tumour removal surgery, we have reviewed a few similar cases in the medical literature. This work has been reported in line with the SCARE criteria [3].
Case presentation
A 33-year-old Iranian female complaining of dull abdominal pain, mainly in the right lower quadrant, referring primarily to the umbilical region and epigastrium was presented to the surgical emergency department. She had also been suffering from another pain in her right flank and a mass sensation while bending her right side. The pain had a colicky pattern with a frequency of almost every 5 min. Nausea and loss of appetite were other symptoms concurrent with the main complaint that also had begun with the abdominal pain. She denied any vomiting. Although the patient remarked foamy, watery defecations with tenesmus during the recent 2 months, she had not had any evacuation or gas passing since the day before admission. She had a 4-year history of coeliac disease (CD) and anaemia, besides colon cancer in her father. Upper endoscopy revealed only decreased duodenal folds, and the biopsy confirmed the celiac disease. Ultrasonography detected a hypoechoic mass 26 × 17 × 27 mm in diameter right anterolateral to the aorta in the level of renal arteries regarding lymphadenopathy. At the same time, an abdominal CT scan reported a solid cystic mass in the paracolic region with a primary diagnosis of intussusception beside mild intestinal loops’ dilatation (Fig. 1). She underwent midline laparotomy with the preoperative diagnosis of gastrointestinal obstruction. After evacuating nearly 500 ccs of reactive serosal fluid from the abdomen, a sizeable ascending colon tumour completely obstructing the lumen attracted the operating team (Fig. 2). There was also intestinal distention and a jejunojejunal intussusception 45 cm away from the mass accompanied by diffuse mesocolonal lymphadenopathies (Fig. 3). Due to its severe attachment to the terminal ileum, ascending and transverse mesocolon, fixing it to retroperitoneum, they tended to right hemicolectomy contemporary with all regional lymph nodes dissection. The primary end-to-end anastomosis between the ileum and the remaining transverse colon was done in two layers. Then, the jejunojejunal intussusception with a margin of 10 cm from both sides was removed. Pathologic study revealed the synchronous adenocarcinomas of large and small intestines; a polypoid mucinous-type well-differentiated adenocarcinoma of the colon with mesenteric lymph node and vascular involvement contemporary with round shaped moderately differentiated adenocarcinoma of the jejunum. She was introduced to the oncologist for chemoradiotherapy. The weekly follow-ups to a month and then monthly once up to 6 months were uneventful. The events are listed in the diagram.

The axial CT scan slices of the case showing a target-shaped view (thick arrow) introducing intussusception and a distended obstructed colon with fluid accumulation distal to it due to a large mass of colon (thin arrows).

The jejunojejunal intussusception.
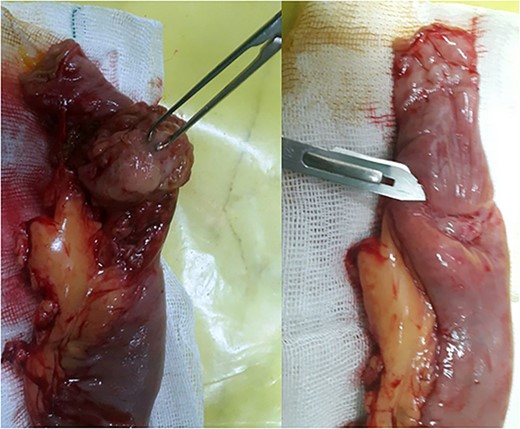
The intraluminal intestinal mass before (pointed by bisturi blade) and after dissection (grasped by Allis tissue forceps).
Discussion
The more common in children, the rarer intussusception is found in adults with an approximate ratio of 20:1. Epidemiologically, in this population, it is seen around two to three cases per million per year [4] account for <5% of all cases of intussusception and 1% of patients with bowel obstruction patients [5]. This phenomenon occurs when a proximal segment of the intestine invaginates with the distal neighbour in a telescoping style. For this, a barrier is needed opposite of peristaltic action forces so that the reaction causes invagination of the two adjacent intestinal parts. Any intestinal condition that intervenes in the natural peristalsis pattern may increase the risk of intussusception. These lead points can be located in the intestinal lumen, within the wall or extramural [6]. Whether malignant or benign, masses are responsible for 60% of cases with the lead point. The remaining non-idiopathic cases are usually due to bowel adherences, Crohn’s disease, infections, intestinal ulcers, and Meckel diverticulum [7], which are common in inflammatory nature. The CD is as common as approximately 1–2% prevalent in North and South America, North Africa, India, and the Middle East [8]. In the paediatric population, mesenteric lymphadenopathies almost do the role mentioned above. However, in adult cases, the malignant masses should be in mind. Although controversial, the management of adult intussusception requires consideration in four aspects: (i) the underlying disease, its frequency, and the need for surgical intervention; (ii) the track of malignancy and further operations; (iii) the anatomy and extension of intussusception; and (iv) any inflammatory condition, oedema, or bowel ischemia [9]. Intussusception is responsible for 1% of bowel obstruction causes in adults, representing 5–10% of intussusception cases in the whole age range [10]. Although the association between CD and increased risk of gastrointestinal malignancies has been proved, their underlying pathophysiology has not already been cleared [1, 11]. A meta-analysis paid this association, and its results indicated that CD increased various malignancies and GI, particularly oesophageal and small intestinal cancers [12]. The correlation among GI cancer, CD, and intussusception can be discussed in three concepts: (i) an intestinal mass in the way of peristalsis can be a lead point for intussusception; (ii) CD increases the risk of malignant tumours, primarily intestinal lymphoma, or adenocarcinoma; and (iii) there are some relationships between CD and recurrent intussusceptions in adults. The intestinal invagination in CD patients is typically non-obstructive, transient, and recurrent [13]. However, our patient was presented to the emergency department with a history of paraclinical intestinal obstruction. The rarity of small intestine carcinoma justifies an annual incidence of 0.66 cases per 100 000 person-years in the United States. Its male to female ratio is about 1:1.45 [14]. Patients with CD have a ten times greater risk of getting intestinal adenocarcinoma than the general population [15]. Although not proven, the carcinogenesis mechanisms in CD are supposed to interfere with genetic factors, environmental carcinogens, chronic inflammation, chronic antigenic stimulation, the release of pro-inflammatory cytokines, and nutritional disorders [13]. Abdominal pain is CD’s most common symptom of intussusception [16]. Obstructive symptoms, nausea, vomiting, and smooth abdominal mass palpation stand in the following steps. We have found only two articles with the keywords ‘Synchronous’, ‘adenocarcinoma’, and ‘Coeliac disease’ in the literature, searching PubMed/Medline, Google Scholar, and Web of Science. The first report, published in 2003, was about an old female complaining of persistent vomiting, crampy abdominal pain, diarrhoea, and underlying iron deficiency anaemia. Her CD was diagnosed 9 years before, and her final diagnosis was complicated synchronous and metachronous jejunal adenocarcinomas without intussusception [17].
Conclusion
Intussusception in adults should warn physicians about the malignant probability of lead points or an underlying inflammatory process involving the bowels. This work indicates the aspects of the first intestinal adenocarcinoma, which can be a lead point for adult intussusception. The second, CD alters intestinal motility and may lead to intussusception; the third, the chronic inflammation caused by the CD can increase the risk of intestinal malignancies.
Conflict of interest statement
None declared.
Funding
None declared.
Ethical approval
This issue has been raised and approved by the ethics committee of Ardabil University of Medical Sciences, Iran.
Consent
The consent in which the patient can use medical records and therapeutic information is attached to the medical document. The authors testify to patient privacy maintenance. On request, a copy of the written consent is available for review by the editor-in-chief of this journal. The authors ensure that all the images/figures/photos are suitably anonymised with no patient information or means of identifying the patient.
Research registration
Since this case report contains no new surgical technique or equipment, it has no Research Registry UIN.
Provenance and peer review
Not commissioned, externally peer-reviewed.

{kind=link}
{kind=link}
{kind=link}