





Abstract
Herein, we report a 48-year-old male with lipofibromatous hamartoma-induced secondary carpal tunnel syndrome, treated successfully with decompression. The patient presented to the emergency with complaints of paresthesia and oedema of the wrists. When non-invasive methods failed to ease symptoms and nerve damage became a big concern, surgical intervention was recommended. Surgery to remove the nerve sheath and expose the carpal tunnel alleviated pressure on the median nerve. After a 3-year follow-up, the patient reported no discomfort, paresthesia, or limitation in wrist or finger movements, indicating a remarkable recovery. The tumour did not recur, and the sensorium was unharmed.
Introduction
Lipofibromatous hamartoma (LFH) is a rare, benign peripheral nerve tumour characterized by excessive fibro adipose tissue growth infiltrating the epineural and perineural components [1]. Although the median nerve in the carpal tunnel is the most frequent target of LFH, other nerves, including the ulnar, radial, sciatic, and plantar nerves, are also susceptible to compression. Macrodactyly is one of the several congenital disabilities linked to LFH’s congenital genesis [2].
Case presentation
A 48-year-old man with a history of epilepsy successfully managed with sodium valproate appeared with swelling of the volar left wrist, discomfort in the radial three fingers, and paresthesia in the thenar region. The patient was tentatively diagnosed with a ganglion cyst pressing on the median nerve, which would explain the patient’s symptoms. The patient reported a 2*1 cm soft lump on the volar aspect of his wrist that extended to the palmar side of his hand. A thorough neurological evaluation showed normal distal pulses, capillary refill, and intact sensory and motor functioning of the radial, ulnar, and median nerves. Tinel and Phalen’s testing showed no signs of thenar atrophy. Ultrasound imaging showed a hyperechogenic lesion measuring about 2*0.64 cm adjacent to the left wrist with no vascular activity. The skin had thickened at the bottom of the left thumb into a roughly 0.51*0.84 cm lesion. The magnetic resonance imaging (MRI) scans showed an abnormally expanded median nerve with a ‘coaxial cable’ or ‘spaghetti-like’ appearance due to its enlarged cylindrical fascicles with a central intermediated focus in T1 and relatively high signal intensity in T2, surrounded by fat (Fig. 1). Histopathological confirmation of the MRI diagnosis of a tumour in the nerve sheath or a fibrolipomatous hamartoma of the median nerve was deemed necessary. Surgery to relieve pressure on the median nerve, including removing the protective sheath and opening the carpal tunnel, was scheduled for a day. During the operation, the incision was prolonged proximally to include the mid-forearm and the distal palmar crease, demonstrating that the lesion’s borders extended into the median nerve. The lesion was safely isolated, whereas the nerve sheath was removed (Fig. 2). The wound closure was difficult, but it was accomplished. The patient was substantially less symptomatic after surgery, and he was monitored for three years. At the time of the most recent checkup, the patient had a full range of motion in his wrists and fingers, and his sensorium was unimpaired (Fig. 3). According to nerve conduction testing, significant axonal damage in the median nerve at the wrist and fingers indicated severe left carpal tunnel syndrome.
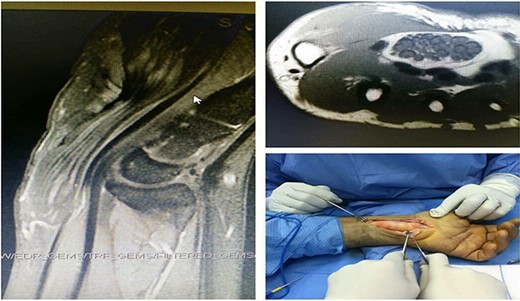
Ultrasound imaging showed a hyperechogenic lesion adjacent to the left wrist; MRI scans showed an abnormally expanded median nerve with a coaxial cable or spaghetti-like appearance.
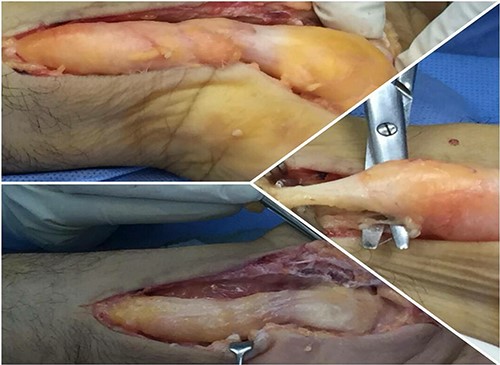
The removal of LFH from the patient wrist.

Range of motion in patient wrists and fingers after recovery.
Discussion
LFH accounts for <5% of benign tumours. LFH is a soft, non-tender lump in young people’s volar aspect of the hand, wrist, or forearm [3]. LFH may be caused by faulty development of the flexor retinaculum in children, trauma, persistent nerve irritation, or hereditary susceptibility. LFH seldom occurs beyond the third decade and is rare but more common in Caucasian people [4]. LFH causes a soft lump, digital hypertrophy, and paresthesia. The tumour’s infiltrative nature might cause median compressive neuropathy on physical examination [5].
Moreover, ultrasonography and computed tomography aid in LFH diagnosis. The ultrasonography shows an expanded hypoechoic median nerve with echogenic substratum and coaxial cable-like bundles. Yet, MRI is preferred for precise diagnosis, surgical planning, and avoiding biopsy since MRI can show serpiginous hypointense nerve fibres (coaxial cables) interlaced with extensive T1/T2 hyperintense fatty tissue along the median nerve [6]. Additionally, compressive symptoms and nerve damage determine LFH treatment. To relieve nerve pressure, early surgical decompression is advised [4]. Surgical excision, micro nerve dissection, and sural nerve graft repair followed by rehabilitation have shown encouraging results [3]. Ganglion cysts, lipomas, and carpal tunnel syndrome should be recognized from LFH in the differential diagnosis. Also, considers traumatic neuroma, neurofibroma, schwannoma, inherited hypertrophic interstitial neuritis, and vascular abnormalities [6].
Conclusion
This case exhibits the efficacy of surgical decompression or excision as a feasible treatment option for LFH that may lead to a beneficial long-term outcome and preserve nerve function.
Conflict of interest statement
The authors declare no potential conflict of interest.
Funding
None declared.
Data availability
Data will be available upon request.
Ethical consent
Written informed consent was obtained from the patient for the publication of this article and the accompanied images.

{kind=link}
{kind=link}
{kind=link}