





Abstract
Acute massive gastric distension is a rare but potentially life-threatening surgical complication of bulimia nervosa. This results from repeated binge eating and is likely compounded by increased gastric compliance and delayed gastric emptying. We describe a case of acute massive gastric distension in a 26-year-old female with undiagnosed bulimia nervosa who underwent a laparotomy and anterior gastrotomy after failed conservative measures for gastric decompression. It highlights the importance of early recognition of a potentially life-threatening condition and that a multi-disciplinary approach is necessary to prevent the recurrence and morbidity associated with it.
INTRODUCTION
We report a case of acute massive gastric distension in a 26-year-old female with undiagnosed bulimia nervosa.
CASE REPORT
The patient presented with acute abdominal pain and distension with an inability to vomit after a large binge, consisting of litres of rice, noodles, vegetables, meat, drinks and dessert, at a ‘hotpot’ restaurant. She appeared distressed and was unable to lie flat, with examination revealing gross abdominal distention. She had an unremarkable routine laboratory workup, including a normal white cell count and lactate level. She received fluid resuscitation. An 18 French nasogastric tube was inserted successfully into the stomach, but no gastric content was able to be aspirated. A computed tomography (CT) of the abdomen and pelvis demonstrated a well-positioned nasogastric tube within a grossly distended stomach that passed inferiorly below the level of the pelvic brim, occupying most of the abdominal cavity (Fig. 1). The pylorus and duodenum were collapsed, demonstrating no passage of food distally. There was no imaging evidence of perforation.
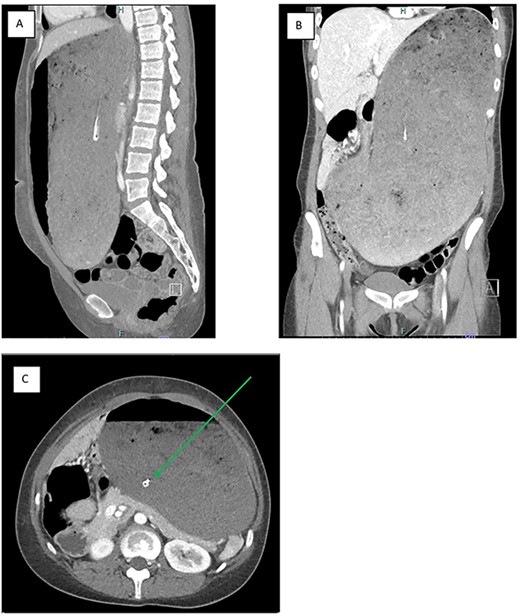
a CT image of the gross gastric distension extending into the pelvis secondary to a binge episode in the (A) sagittal, (B) coronal and (C) axial slices; the nasogastric tube (green arrow) is appropriately placed within the gastric lumen
She was taken to the operating theatre due the risk of potential gastric ischemia secondary to prolonged gastric distension. An upper midline mini-laparotomy and anterior gastrotomy was performed to evacuate the approximately 5 litres of food content consisting of poorly masticated meat, noodles, rice and vegetables. There was no evidence of ischemia. The gastrostomy was closed in two layers.
The patient’s post-operative course was unremarkable. The nasogastric tube was removed the following day and the patient was commenced on a fluid diet. She was reviewed by a multi-disciplinary team, including a psychiatrist, psychologist, dietitian and social worker. Psychological review revealed that she had regularly undertaken bingeing and purging and had very poor insight into the harms associated with her behaviour despite it having resulted in surgical intervention at this admission. After ensuring she had sufficient social supports, she was cleared by the psychiatrist and was discharged home on the fifth post-operative day with outpatient follow-up.
DISCUSSION
This case highlights the potentially acute life-threatening surgical implications of bulimia nervosa. Bulimia nervosa typically manifests, in patients of normal weight, as recurrent episodes of uncontrollable binge eating, followed by compensatory behaviour to prevent weight gain, including purge vomiting, laxatives, diuretics or excessive exercise [1]. Most medical complications relate to the compensatory phase, such as dental erosion, gastroesophageal reflux or oesophagitis, electrolyte imbalances and dehydration from laxative or diuretic abuse [2]. However, the binge phase of this condition can also lead to surgical complications as demonstrated here.
Reports of acute gastric dilatation in patients with eating disorders have been in the literature since the 1970s [3]. While it can be seen in both anorexia nervosa and bulimia nervosa, most of the literature pertains to patients with anorexia nervosa. In bulimia nervosa, this results from large binge of food with build-up of gastric, biliary and intestinal secretions, compounded by increased gastric compliance and delayed gastric emptying noted in patients with binge-eating disorders [4]. Severe cases of acute gastric distension have resulted in full thickness necrosis requiring partial or total gastrectomy [5, 6]. Lethal outcomes, including from abdominal compartment syndrome as a result of severe gastric distension, have also been reported [7–9].
In this case, it is likely that there has been chronic gastric distension from previous binge episodes which allowed the stomach to be grossly distended without ischemia or perforation. Anorexic patients seem to have much longer gastric emptying times for solid food compared to the normal population but not for liquids. There have also been studies showing a diminished sensitivity to gastric distension in patients with bulimia nervosa [10], hence allowing the stomach to distend to a dangerous size before becoming symptomatic. This condition requires early recognition of a potentially life-threatening complication and early surgical intervention if concerns of gastric ischaemia exist.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}