





Abstract
Nasogastric tubes (NGT) are widely used and generally harmless as such, complications are uncommon. NGT knotting is one such complication. We report a 45-month-old female with spontaneously knotted NGT that was identified and safely removed without complications. NGT knotting detection needs a high index of suspicion; if not detected and managed in a proper way, it may lead to severe complications. We discuss this case to raise awareness of this complication and how to minimize the likelihood of it happening and improve patient outcome.
INTRODUCTION
Nasogastric tubes (NGTs) are commonly used in medical practice and even more so in surgical patients. Most frequent indications are feeding and decompression. Although relatively less invasive, they are not free from complications ranging from minor mucosal trauma to fatal hydrothorax and empyema [1]. Unprompted knotting of the tube is uncommon and even rarer in children and if undiagnosed can cause serious unsuspected trauma.
CASE REPORT
A 45-month-old female presented to the Accident and Emergency department (A&E) with a 2-week history of fever and non-productive cough. Her condition had worsened 2 days prior presentation at the A&E with irretractable fevers, projectile vomiting, decreased mentation and two episodes of generalized tonic clonic convulsions. On systemic examination, the child had a Glasgow Coma Score (GCS) of 6/15.
The patient was admitted to pediatric intensive care after brain CT, chest X-ray, gastric aspirate and Cerebrospinal Fluid (CSF) for GeneXpert® as well as blood works confirmed diagnoses of extra pulmonary tuberculosis (EPTB)—tuberculous (TB) meningitis; severe anemia; severe acute malnutrition and severe hyponatremia.
A 12 Fr NGT and an 8 Fr urethral catheter were inserted by an assistant nursing officer after lubricating with a surgical lubricant. Correct placement of NGT was verified by injecting about 10 cc of air while auscultating the epigastrium. The patient was successfully started on feeds and treatment via NGT without any complication. Over the next 30 days, the patient’s GCS improved as such the orders during ward rounds were to change the NGT and the urethral catheter (and thereafter routinely after every 2 weeks). Prior multiple failed attempts to remove it, the NGT was noted to be in situ beyond the usual length however, knotting was not suspected as the NGT allowed feeds to pass through. The patient was sent for a chest and abdomen X-ray, which showed the NGT knotted in a figure-of-8 pattern and was subsequently removed endoscopically (Fig. 1).
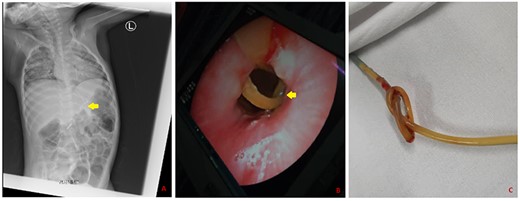
Knotted NGT as seen on a plain radiograph (A), endoscopy (B) and after removal (C).
DISCUSSION
The use of NGT in the pediatric population is very frequent for both medical and surgical indications. Insertion and removal of the tube are both straightforward procedures albeit with high risk of complications if not performed carefully [2].
Complications due to NGT may be divided into nasal complications (ulceration, epistaxis), esophageal complications (erosion and perforation), pulmonary complications (aspiration, bronchial and lung injury) and tube-related complications (tube breakdown and knotting) [3]. To the best of our knowledge, there are less than five reported cases of NGT knotting in the pediatric population [4–6].
Although an uncommon entity, NGT coiling or knotting remains one of the numerous complications that emerge after or during tube placement. There are some causes that predispose NGTs to loop formation. One of them is the thin lumen and malleability as well as excessive insertion of tube [7]. Swallowing or coughing may also lead to NGT coiling or knotting [8].
In this case, two risk factors seem to account for the knotting: chronic cough and redundant NGT in the gut noted both clinically and on abdominal X-ray. On the contrary, the theory of thin lumen as a risk for knotting could not be supported in this case given that an age-appropriate and fitting (12 Fr) NGT was inserted in the patient.
The resistance experienced during the removal of the tube increases progressively as the catheter passes through the narrowest part of the esophagus however, when it fails to come out or any doubt exists, a radiograph should be done to check the position of the NGT [9]. Forceful removal may cause occlusion or injury to the airway leading to fatal complications.
CONCLUSION
This case report highlights and reminds healthcare workers that no procedure is small and should not be taken lightly in view of its simplicity. It demonstrates that even a routine procedure such as the insertion of a NGT can have potentially serious consequences as such all principles should be adhered to when performing such procedures. Awareness of possible complications related to the NGT will help avert them and improve patient outcomes. Only the necessary length of tube should be inserted. A usually accurate length can be determined by measuring tubing required, prior to insertion. This is practically done by tracing an imaginary course from the nostril, looped round the ear or along the side of the face past the ear and then to the xiphoid process. The neck is in anatomical position. An allowance of about 5 cm may be added for proper function [8].
ACKNOWLEDGMENT
We are grateful to the patient’s mother for consenting to the use of patient’s case notes and images for this publication.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
References
Ismail NJ, Bot GM, Hassan I, Shilong DJ, Obande JO, Aliu SA, et al.
Galanopoulos M, Tsigaridas A, Varytimiadis L, Papaefthymiou A, Kalampalikis L, Ladias S, et al.

{kind=link}