





Abstract
Scrotal lipoma is a type of rare benign mesenchymal tumor. These lipomas can masquerade as inguinal hernias that can cause surgical dilemmas. The size of lipomas can vary, with some growing into remarkably large masses. We present a case of a 75-year-old male with a history of laparoscopic hernia repair, who noticed a progressively enlarging left scrotal bulge. An open hernia repair procedure was performed, unexpectedly revealing two large left-sided scrotal masses, which were subsequently excised. Based upon the histopathologic findings of these masses, scrotal lipomas with fat necrosis were diagnosed.
INTRODUCTION
Scrotal lipoma is a type of benign mesenchymal tumor. These lipomas can masquerade as inguinal hernias that cause surgical dilemmas. The size of these lipomas can vary from 1 cm to >10 cm [1]. We present a case of a 75-year-old male with two large left scrotal lipomas.
CASE REPORT
A 75-year-old male with a history of laparoscopic left inguinal hernia repair many years ago presented for evaluation of progressively enlarging left scrotal bulge for the last 3 years that was associated with minimal pain. The patient’s clinical presentation appeared to be that of a recurrent left inguinal hernia with incarcerated omentum within the scrotum. He subsequently underwent open hernia repair. Once the external oblique aponeurosis was opened, exploration revealed no evidence of a recurrent hernia. Two masses were felt in the proximal scrotum and they did not communicate with the spermatic cord. The scrotal masses were isolated; via the inguinal incision and excised for pathologic diagnosis. The patient had no operative or postoperative complications and showed good healing at his 3-week follow-up visit.
PATHOLOGIC ANALYSIS
Grossly, the two masses appeared to consist of mature, encapsulated lobulated adipose tissue. They measured 10 × 5.5 × 4.2 cm and 10.3 × 5.2 × 4.2 cm and collectively weighed 199 g. Serial sections of each specimen revealed similarly appearing yellow, greasy, lobulated adipose tissue with focal, pale yellow/tan nodules suggestive of fat necrosis.
Histopathologic evaluation of representative hematoxylin and eosin (H&E)-stained sections from each specimen were similar and showed mature adipocytes of typically uniform size with foci of degeneration of fat necrosis. Adipocytes did show varying sizes in these regions of necrosis and degeneration. The tumors exhibited the typical fibrous septal vascularity of mature, benign lipomas. Rarely, focal microcalcifications are seen in areas of fat necrosis with degenerative adipocyte changes (Figs 1 and 2).
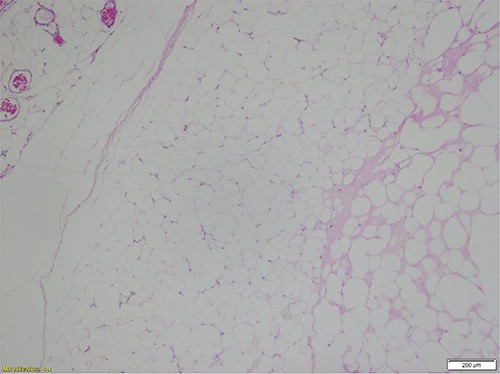
Mature adipocytes of a benign lipoma with relatively scant, septal vascularity and foci of fat necrosis (H&E-stained section; ×40 total magnification: ×4 objective with ×10 ocular lens) (Courtesy Karl Biesemier, MD. Pathology Consultants of Central Virginia, Lynchburg, VA).
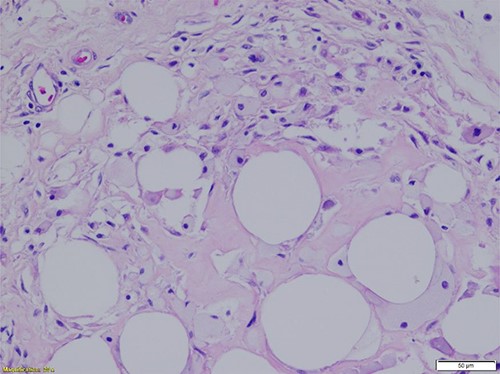
Region of fat necrosis within the benign lipoma. Scattered inflammation and focal degenerative adipocyte changes are seen along with rare microcalcifications (H&E-stained section, ×200 total magnification: ×20 objective with ×10 ocular lens) (Courtesy Karl Biesemier, MD. Pathology Consultants of Central Virginia, Lynchburg, VA).
DISCUSSION
Scrotal lipomas are the most common benign mesenchymal tumor of scrotal tissues and the spermatic cord in all age groups [2, 3]. Scrotal lipomas generally are classified into three categories: (i) subcutaneous fatty tissue posterior to the spermatic cord and extending into the scrotum (called scrotal lipomas), (ii) adipose tissue within or outside spermatic cord (called spermatic cord and tunica vaginalis lipomas) and (iii) fat lobules within the scrotal dartos tunica (called primary scrotal lipomas) [1, 4]. Spermatic cord lipomas are the most common and can be found in 20–70% of inguinal repairs [5]. On the contrary, primary scrotal lipomas are rare and occur more often in young males, whereas the other two categories occur more commonly in men between 40 and 60 years old [1, 6]. The precise location of lesion origination is difficult to identify [2, 6]. The sizes of scrotal lipomas have been reported in wide ranges up to 9000 g [2, 7]. Clinically, patients may report a sensation of scrotal fullness, without signs of trauma or inflammation. Upon physical examination, lipomas may mimic an inguinal hernia, which may cause unexpected intraoperative findings [2, 3, 7, 12]. The treatment of choice is surgical removal with histologic diagnosis, which is crucial to rule out malignancy, such as liposarcoma or leiomyosarcoma [1, 2, 4, 8].
Pathophysiology
Lipomas can be located anywhere where normal adipocytes are present in the body. Most of the time, they occur in the subcutaneous layer but could also extend to fascia or muscle layers. The incidence is higher in patients with obesity, hyperlipidemia and diabetes mellitus [9]. The exact pathogenesis of lipomas remains unknown. However, trauma has been hypothesized as a cause. It is thought that trauma incites a release of pro-inflammatory cytokines that subsequently cause immature adipocyte to differentiate and mature. There is a potential genetic linkage to acquiring lipomas, especially in patients with multiple lipomas. The most common cytogenetic mutations identified thus far involve chromosome 12q13-15, resulting in the fusion of the high-mobility group AT-hook 2 (HMGA2) gene with various transcription regulatory domains leading to the formation of tumors. Deletion of 13q and rearrangement of 6p21-33 are the second and third most common genetic abnormalities found, respectively. Histologically, lipomas appear indistinguishable from mature normal adipocytes of subcutaneous tissue. There are various histologic variants of malignant lipomatous neoplasms (liposarcomas). Malignant adipocytes show clear variation in size and at least focal cytologic atypia and nuclear irregularity or hyperchromasia. The hyperchromatic stromal cells tend to be more numerous in the fibrous septa. Varying numbers of monovacuolated or multivacuolated lipoblasts may be seen. Lipoblasts are commonly considered to be the hallmark of any of the histologic variants of liposarcoma. Clinical consequences of lipoma vary based on their sizes and locations. Visceral (or internal) lipomas are most commonly found in the gastrointestinal tract, specifically in the ileum in geriatric patients. As a result, they can obstruct the lumen, causing bleeding, jaundice and pain. In younger patients, lipomas can cause intussusception [9–11].
CONCLUSION
Scrotal lipomas are benign tumors that may present clinically like inguinal hernias. Surgical resection to include the complete fibrous capsule of the neoplasm remains the treatment of choice to prevent reoccurrence. Histopathologic evaluation is essential for diagnosis and to rule out atypical features or malignancy [8, 9].
CONFLICT OF INTEREST STATEMENT
None.

{kind=link}
{kind=link}