





Abstract
Intraocular foreign bodies (IOFBs) are the most common emergency cases in ophthalmology causing severe visual impairment to blindness. We present nine male patients with IOFBs, aged 28–64 years old, which displayed a wide spectrum of findings. Based on IOFB location, four cases were intravitreal, two were intraretinal, two were intralenticular and one was intracorneal. The most common material was metal, from hammering projectiles (six patients). The injuries mainly occurred at workplace (five patients). All IOFBs were successfully extracted. Initial visual acuity (VA) ranged from light perception to 20/32; six patients had better final VA, up to 20/20. A wide range of ocular manifestations is associated with IOFBs. Removing retained IOFB procedure is dependent on location, nature, lens opacity and vitreoretinal involvement. Meticulous ocular examination and imaging modality are vital to identify the IOFB presence. Various visual outcomes depend on zone involvement, IOFB size and level of difficulties of surgery.
INTRODUCTION
Penetrating ocular injury with intraocular foreign bodies (IOFBs) is a type of injury that may result in severe ocular tissue damage and visual loss. IOFBs account for 17–41% of open globe injuries [1, 2], and about 70.3% posterior segment injuries lead to blindness [3]. IOFBs could trigger complications including hyphema, cataract, vitreous hemorrhage and retinal tear and detachment [4]. Certain metallic foreign body within the eye may produce retinotoxic ions, e.g. siderosis and chalcosis [5], and most metallic IOFB should be removed promptly to prevent these reactions and minimize intraocular inflammation [6]. Timing of surgery for IOFB removal is controversial, about 88% patients were reported blind due to delayed procedures (>24 h) [3]. Other indication to remove IOFB promptly is to prevent endophthalmitis that may result in blindness [6]. Therefore, some authors advised IOFB removal within 24 h to provide good outcomes [3, 5, 7]. A good patient history-taking and a thorough ocular examination are still most important factors for diagnosing IOFB [6]. Radiological investigations such as plain orbital X-rays, ocular ultrasonography, computed tomography (CT) and magnetic resonance imaging can be used to detect and localize IOFBs [8]. We present the mechanisms of injury, ocular presentations, management and visual outcomes in nine cases of penetrating open globe injury patients with IOFB.
CASE REPORT
A total of nine patients were presented in this case series, the data were collected from 2012 to 2019 at two private eye hospitals in Jakarta. All patients were male, with mean age of 42.44 ± 12.78 (ranged 28–64 years old). Almost all injuries were unilateral (eight patients) and only one patient had bilateral injury (Case 8). The mean time interval between injury and presentation was 7.7 ± 10.5 days (ranging from 6 h to 1 month). The injuries most commonly occurred at workplace (five patients) followed by home (three patients) and on the road or related to motor vehicle accident (MVA), in one patient. Upon presentation, the patients had a broad spectrum of initial visual acuity (VA), ranging from 20/32 to light perception (LP) with a mean VA of 1.36 ± 0.83 logMAR. All patients came with various clinical findings from mild to severe presentations, and corneal ruptures found to be the main entry sites of all injuries (Zone 1). Endophthalmitis was reported in two patients (Cases 2 and 3); both were presented to the hospital more than days after the injury. All details are described in Table 1.
Summary and detail of case series
| Description | Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 | Case 7 | Case 8 | Case 9 |
|---|---|---|---|---|---|---|---|---|---|
| Age (year), Gender | 33, Male | 39, Male | 39, Male | 28, Male | 64, Male | 58, Male | 29, Male | 52, Male | 40, Male |
| Laterality | RE | RE | RE | LE | RE | RE | RE | RE and LE | LE |
| Arrival time | 12 h | 3 weeks | 5 days | 5 days | 1 month | 6 h | 5 days | 12 h | 2 days |
| Place of injury | Home | Workplace | Workplace | Workplace | Workplace | Home | Workplace | Road | Home |
| Initial VA | 20/200 | LP | LP | 20/32 | CF | 20/125 | 20/63 | RE 20/63, LE CF | CF |
| Ocular Presentation | Corneal rupture | Corneal rupture with three sutures, shallow AC, hypopyon and fibrin, traumatic cataract, lens fragment in AC, irregular pupil, vitreous hemorrhage, endophthalmitis | Self-sealing corneal rupture, hyphema with fibrin, traumatic cataract, endophthalmitis | Corneal rupture, traumatic cataract, intraretinal hemorrhage | Corneal haze, self-sealing corneal rupture, entry wound in iris, irregular pupil, traumatic cataract | Corneal rupture, traumatic cataract, vitreous hemorrhage, retinal detachment | Corneal rupture, iris rupture, traumatic cataract, vitreous hemorrhage, giant retinal break | Corneal rupture, iris prolapse, traumatic cataract | Corneal rupture, traumatic cataract, vitreous hemorrhage, retinal detachment |
| IOFB: (detection, material, and mechanism) | Slit lamp Glass, blast | During surgery Stone particle, projectile | B-Scan USG Metallic iron, projectile | Funduscopy, CT scan Metallic iron, projectile | B-Scan USG Metallic iron, projectile | During surgery Metallic iron, projectile | Plain orbital X-Ray Metallic iron, projectile | Slit lamp Glass, MVA | During surgery Metallic iron, projectile |
| Zone, IOFB location | Anterior, cornea | Posterior, vitreous | Posterior, retina | Posterior, retina | Anterior, lens | Posterior, vitreous | Posterior, vitreous | Anterior, lens | Posterior, vitreous |
| Size | 2 × 1 mm | 0.5 optic DD | 0.5 optic DD | 3 × 5.5 mm | 1 × 1 mm | 1.5 optic DD | 4 × 3 mm | 3 × 2 mm | 1.5 optic DD |
| Management | Corneal repair, IOFB extraction | Lensectomy, PPV, endolaser with silicone oil tamponade, IOFB extraction | Intravitreal antibiotics, lensectomy, PPV, endolaser with silicone oil tamponade, IOFB extraction | PPV, endolaser with silicone oil tamponade, IOFB extraction | IOL Phacoemulsification, IOFB extraction | IOL Phacoemulsification, PPV, endolaser with silicone oil tamponade, IOFB extraction | I/A lens, PPV, endolaser with silicone oil tamponade, IOFB extraction | Corneal repair, IOFB extraction, lens extraction | IOL Phacoemulsification, PPV, endolaser with silicone oil tamponade, IOFB extraction |
| Last VA | 20/20 | HM | 20/200 | LP | 20/40 | 20/25 | HM | RE 20/50, LE HM | CF |
| Complication | None | None | PVR, postoperative retinal detachment | phthisic eye | None | None | None | Secondary glaucoma | None |
AC, anterior chamber; CF, counting finger; DD, disc diameter; HM, hand movement; IOL, intraocular lens; I/A, irrigation/aspiration; LE, left eye; LP, light perception; PPV, pars plana vitrectomy; RE, right eye; USG, ultrasonography.
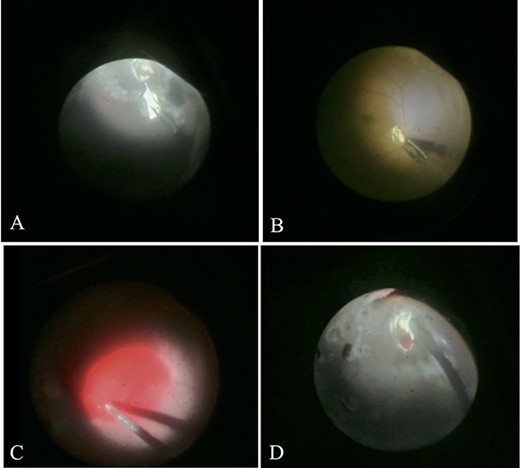
All IOFBs were successfully identified using slit-lamp biomicroscopy, fundus examination, B-scan ultrasonography, plain orbital X-ray, and viewed intraoperatively. Most foreign bodies were intravitreal (four patients, Fig. 1), followed by intraretinal (two patients, Fig. 2), intralenticular (two patients, Fig. 3) and intracorneal (one patient, Fig. 4).
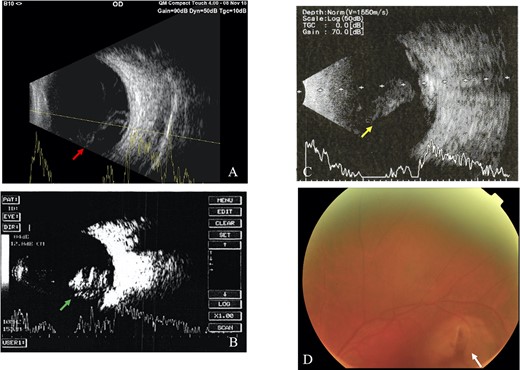
Intravitreal foreign body; (A) B-scan ultrasound revealed vitreous hemorrhage with retinal detachment in Case 6 (red arrow), (B) vitreous hemorrhage in Case 7 (green arrow), (C) vitreous hemorrhage with retinal detachment of the LE in Case 9 (yellow arrow), (D) fundus examination showed hazy vitreous with a retinal tear (white arrow) near superior temporal arcade of the retinal artery (Case 9).
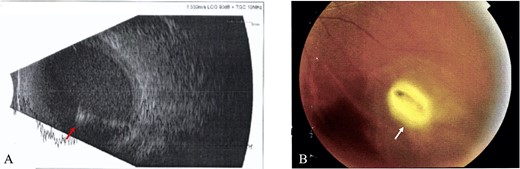
Intraretinal foreign body; (A) B-scan ultrasound revealed hazy vitreous with absence of retinal detachment and high reflective intravitreal object (red arrow), suggestive of metallic IOFB and endophthalmitis (Case 3), (B) Fundus examination showed a foreign body at inferior temporal quadrant of the LE (white arrow), with intraretinal hemorrhage (Case 4).
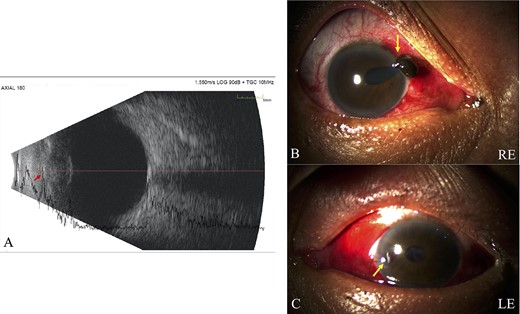
Intralenticular foreign body; (A) B-scan ultrasound confirmed lens opacity, intact posterior capsule and suspected lenticular IOFB (red arrow), with normal vitreous and retina of the RE (Case 5), (B) Slit lamp bio-microscopy revealed corneal rupture and iris prolapse (Zone I) at 2 o’clock limbal, flat AC and traumatic cataract on the RE, (C) corneal rupture (Zone I) at 9 o’clock paracentral, shallow AC and traumatic cataract on the LE were discovered in Case 8 (yellow arrow).
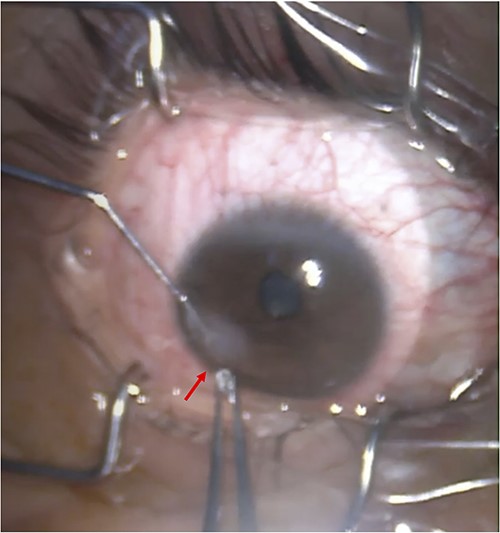
Intracorneal foreign body; a glass fragment in the size of 1 × 1 mm was embedded in the RE cornea and was completely removed using forceps (Case 1).
The most common IOFB material was metallic (iron) in six patients due to projectile hammering; two patients were injured by glass fragment (blast and MVA, respectively) and one patient by projectile stone particle. All patients underwent surgeries, and even though there were some difficulties during the extraction, all IOFBs were successfully removed. In Case 4, the IOFB fell twice on to the retina, causing retinal hemorrhage. Two retinal breaks were observed; one break was at inferior temporal; one iatrogenic break was at perimacular area, which occurred during IOFB removal and caused additional hemorrhage in the vitreous. Finally, it was successfully removed by scleral incision using IOFB forceps, shown as a metallic object with the size of 3 × 5.5 mm. The hemorrhage was controlled, laser barrage was applied and silicon oil 1000 c was injected as tamponade (Fig. 5). Six patients had better final VA, with mean final VA 1.1 ± 0.89 logMAR (ranged from LP to 20/20). Initial and final VA is presented in Fig. 6.
Difficulties during the IOFB extraction in Case 4; (A) A large size metallic iron IOFB was embedded in retina and a retinal break was discovered at inferior temporal, after applied laser barrage to secure the break, the IOFB was removed, (B) The IOFB fell twice on to the retina, but it was successfully removed by scleral incision using IOFB forceps, shown as a metallic object with the size of 3 × 5.5 mm, (C) Retinal hemorrhage after removal was showed and the hemorrhage was managed, (D) One iatrogenic break at perimacular area was found during the removal and caused additional hemorrhage in the vitreous; the hemorrhage was controlled, laser barrage was applied and silicon oil 1000 c was injected as tamponade.
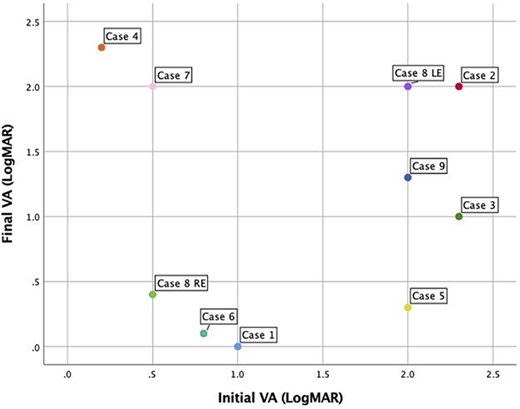
Initial and final VA.
DISCUSSION
Most post-traumatic IOFBs (up to 75%) are known to reside in the posterior segment [9, 10]. This case series demonstrates the vast spectrum of ocular manifestations in eye injury with the presence of IOFB. Intravitreal and metallic iron FB accounts for the most common findings.
Working-age males (28–64 years old) constitute 100% of the patients presenting with IOFBs in our hospital. The predominantly male patients were also shown in other studies [11]. None of our patients were wearing safety glasses or goggles at the time of injury, consistent with a previous study which reported that only 6% of patients wore protective eyewear [12]. The most common place of injury is workplace (5, 55.5%) followed by home (3, 33.3%), as similarly reported by Jonas et al. [11] Projectile mechanism while hammering was documented in seven patients (77.8%), in line with other reports which described hammering (60–80%) as the most common mechanism of injury [11].
A literature review conducted by Loporchio et al. [13] showed that IOFB can enter through cornea (65%), sclera (25%) or at the limbus (10%). This series documented cornea (Zone I involvement) as main entrance of IOFB in all patients. The entry wound in Zone II or Zone II accounted for poor visual outcome (VA <20/400) as reported by Zhang et al. [10]. Among our cases, the IOFBs (in six out of nine patients) were retained in posterior segment, while only in three cases were located within anterior segment. Studies reported that IOFBs are mostly seen in the posterior segment (58–88%), followed by anterior segment (10–22%) such as anterior chamber (10–15%) and the lens (2–8%) [3, 7, 13]. Previous studies have shown that eyes with retained anterior segment FB fared better than those with posterior location [14]. This was observed in our series, as patients with anterior segment injury had VA improvement to 20/20 and 20/40 (Case 1 and Case 5, respectively).
The composition of IOFBs varies from organic material (e.g. insect parts and animal hairs), glass, plastic or metals such as zinc, nickel, aluminum, mercury, iron and copper [15]. We reported six patients with metallic iron IOFBs, two patients with glass IOFBs and one patient with stone particle IOFB. Glass IOFBs complicate up to 14% of all IOFB cases and are especially common with MVA and explosions [15]. Nanda et al. [15] reported up to 70% of MVA-associated penetrating ocular trauma have an accompanying glass IOFB present, which was also discovered in this case series (Case 8). The most serious complication of iron-containing retained IOFB is the development of siderosis bulbi [16]. Therefore, IOFBs require prompt evaluation and management; as they may quickly lead to sight-threatening complications [16].
Two patients in our case series (Case 2 and Case 3) presented with endophthalmitis due to the late onset of injury. They were admitted to our hospital 3 weeks and 5 days after the injury, respectively. It is crucial that an IOFB should be detected early and removed within first 24 h after the injury [17]. Failure to diagnose and manage a retained IOFB increases the risk of endophthalmitis, retinal detachment and the longer term risk of siderosis bulbi, potential loss of vision and eye [17].
All primary care physicians as well as ophthalmologists should be aware of the possibility of a retained IOFB in a penetrating ocular injury particularly when there is a history of high-velocity metallic injury [18]. It should be assumed that ocular injuries sustained in these types of settings potentially harbor an IOFB until proven otherwise [19]. Patients sometimes are unaware that a foreign body might have entered their eyes, as seen in Case 5. The patient came with gradual visual loss with previous history of hitting a piece of metal 1 month ago; late presentations such as healed corneal scars or iris heterochromia may aid in diagnosing previously undisclosed trauma.
To avoid missing the diagnosis, a complete and careful ocular evaluation including imaging studies is therefore essential. The diagnosis of an IOFB is often made by direct slit lamp examination or ophthalmoscopy [20], as presented in Case 1, Case 4 and Case 8. Dilated fundus examination can reveal an FB in the vitreous or retina if the media is clear [20]. If the suspected IOFB is not seen, further evaluation using imaging studies is necessary. Imaging modalities for the detection of a metallic IOFB include plain orbital X-ray, CT scan and ocular ultrasonography [21]. In our cases series, all patients with posterior segment involvement underwent B-scan ultrasonography to confirm the presence of IOFBs. Ultrasonography has been shown to be a very valuable tool that can augment the information acquired from other imaging modalities. It is both sensitive and specific for IOFB localization. Farvardin et al. [22] obtained an accuracy of 100% with ultrasonography for IOFB localization. Plain orbital X-rays may be useful, but non-radiopaque are usually missed by this test [23]. In this series, only Case 4 underwent CT scan imaging.
Surgical technique for removal of a retained IOFB is dependent on the site and nature of the IOFB, lens opacity and whether or not the IOFB is embedded in the vitreoretina [24]. Two patients who suffered from glass FB from blast injury (Case 1) and MVA (Case 8) underwent corneal repairs as described in this series. Six patients underwent vitrectomy due to metallic iron and stone posterior segment IOFBs. Extraction through pars plana incision was potentially associated with higher rates of retinal break formation and subsequent retinal detachment [25]. The higher rate was particularly notable with glass IOFBs [25]. Also, following surgical removal, small iron particles can still be released at the inner retinal surface, potentially inducing further retinal toxicity [26].
One patient developed proliferative vitreoretinopathy (PVR) and postoperative retinal detachment (Case 3). Risk factors associated with the development of PVR include the size of the IOFB and the size and number of retina tears [13], which was also demonstrated in our case series. Many studies have shown that PVR is associated with poor visual outcome [27, 28]. Removal of an IOFB in the presence of detached retina is associated with an increased risk of iatrogenic retinal breaks, which in turn can lead to increased risk of postoperative retinal redetachment [29]. The rate of postoperative retinal detachment ranges from 6 to 40% [28].
Better visual improvement following surgery was shown in six (66.7%) patients in this series. Three patients presented with final VA of ≥20/40. Ehlers et al. [30] showed that presenting VA was better than 20/200, was associated with final VA 20/50 or better. A review by Loporchio et al. [13] concluded that the factors for predictive of poor visual outcome included presentation with hyphema, vitreous hemorrhage, hammering metal on metal as a mechanism of injury, culture of a non-virulent organism, the presence of retinal detachment and the presence of endophthalmitis. Location and mechanism of injury are important factors that influence final VA [30]. Injury limited to the anterior segment was found to be predictive of better final VA compared with posterior segment injury [30].
In penetrating ocular injuries, IOFBs mostly enter the eye through corneal wounds, causing a wide spectrum ocular tissue damage and ocular manifestations. Various visual outcomes are identified, depending on Zone of injury, size of IOFB and difficulties during removal. Ocular trauma to the posterior segment accounts for poor prognosis. Careful eye examination and imaging modalities are essential to identify the presence and characteristics of IOFB. Time interval between injury and presentation also play crucial role in planning ocular trauma management.
FUNDING
This case series did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
CONFLICT OF INTEREST STATEMENT
None declared.
PATIENT CONSENT
Patients’ written informed consents were obtained to any case details and any accompanying image published.
ACKNOWLEDGEMENTS
The authors thank JEC Eye Hospitals and Clinics for providing patients’ medical records and Ophthalmic Trauma Service of JEC Eye Hospitals and Clinics.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}