





Abstract
Adenomatoid tumors are incidentally found, rare tumors that are usually benign. They usually originate from mesothelial cells and have been reported to occur in the genital tract, though occasionally occur in extra-genital locations. A 33-year-old African–American female was found to have a large multiloculated cystic lesion in segments IV and V of the liver. The patient underwent a laparoscopic central hepatectomy and the tumor was resected en bloc. On pathologic analysis, the specimen showed multiple cysts of variable sizes lined by a single layer of low cuboidal cells. Immunohistochemistry revealed cells staining positive for WT-1 and calretinin, indicative of a tumor of mesothelial origin. Adenomatoid tumors are rarely, if ever found to occur in the liver. Their malignant potential and biology in the liver is unknown, however given their benign behavior in other organs, resection was considered curative.
INTRODUCTION
Adenomatoid tumors are incidentally found, rare tumors that are usually benign. They originate from mesothelial cells and have been reported to occur in the genital tract. Occasionally, they occur in extra-genital locations such as the adrenal gland, heart, mediastinum, as well as the peritoneal and pleural lining. However, the liver as a primary location for this tumor is extremely uncommon, with less than a handful of cases being reported in literature [1–4]. Due to the rare nature of the pathology, postoperative management of this tumor is not established.
CLINICAL CASE
A 33-year-old African–American female with relevant medical history of morbid obesity, polycystic ovarian disease, history of deep vein thrombosis, pulmonary embolism and prior cholecystectomy presented with right upper quadrant pain. She did not exhibit symptoms of obstruction. Initial evaluation by abdominal ultrasound before presenting to the clinic demonstrated a large polycystic lesion.
Computed tomography (CT) revealed a large multiloculated cystic lesion in segments IV and V of the liver measuring ~21.0 × 14.0 cm (Fig. 1). The mass extended down into the right lower quadrant, causing a mass effect with effacement of the duodenum, vena cava and displacement of the transverse and right colon inferiorly. Due to the recent nature of her cholecystectomy and cystic nature of the mass a biloma could not be excluded. Therefore a hepatobiliary iminodiacetic acid scan was ordered, which did exclude biloma.
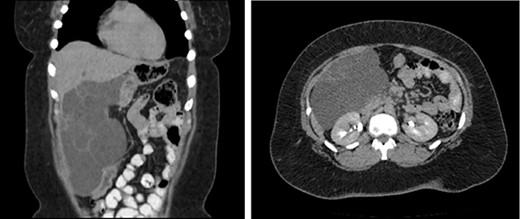
CT of the abdomen and pelvis (coronal, axial) which reveals a septated complex cystic mass displacing the duodenum and vena cava.
The patient underwent a laparoscopic central hepatectomy, for diagnostic as well as therapeutic purposes. Intraoperatively a 15 cm multiloculated cystic neoplasm was found originating in segments IV and V of the liver extending into the retroperitoneum. The tumor was carefully dissected from the retroperitoneum and resected en bloc. Postoperatively, the patient did well and was discharged home on postoperative Day 4.
Pathologic analysis demonstrated multiple cysts of variable sizes surrounded by dense stroma with mild to moderate inflammation. The cysts were lined by a single layer of low cuboidal cells (Fig. 2A). Immunohistochemistry was performed with the cells staining positive for Wilms Tumor 1 and calretinin, indicating mesothelial origin (Fig. 2B). The lesion was classified as an adenomatoid tumor.
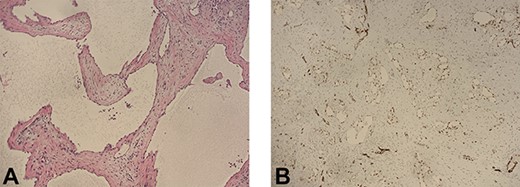
(A) Histopathologic study reveals cystic spaces lined by a single layer of low cuboidal cells (H&E, 10×). (B) The lining cells show positive nuclear staining for WT-1, favoring mesothelial origin.
Follow-up laboratory studies and a CT scan were performed 4 months and 9 months postoperatively for surveillance. All liver function tests were within normal limits and no abdominal mass and lymphadenopathy was seen.
DISCUSSION
When encountered with complex cysts of the liver, differential diagnoses can be diverse and include mucinous cystadenomas of biliary origin, intraductal papillary neoplasms of biliary origin, echinococcal cysts, cystic hepatocellular carcinoma among other rare pathologies [5, 6]. Mucinous cystic neoplasms and intraductal papillary neoplasms of biliary origin have only recently been discovered to be two distinct clinical entities, both with malignant potential [7]. Echinococcal cysts, also known as hydatid cysts, are caused by Echinococcus granulosus infection in endemic regions. Lastly, hepatocellular carcinoma may appear as multilocular cystic lesions of the liver. Ultimately, surgical intervention is indicated in symptomatic cysts or those with suspicious features of malignancy.
Adenomatoid tumors are tumors of mesothelial origin that are have only been encountered a handful of times as a primary tumor in the liver [4]. These benign tumors are most often encountered in the genital tract. In males, they make up 30% of all paratesticular masses and may be encountered in the epididymis, spermatic cord and prostate [8]. In females, they may be found in the uterus and fallopian tubes. When encountered, they are usually asymptomatic, slow growing masses. Resection of the tumor can be both diagnostic and therapeutic. They are not known to recur or have malignant degeneration [8]. Given the biology of the tumor known in other organs and unusual presentation in the liver, postoperative surveillance by CT scan performed 4 months and 9 months out was chosen, without further medical interventions. No recurrence was noted.
CONCLUSION
Adenomatoid tumors are tumors of mesothelial origin that are extremely rare to occur primarily in the liver. Their malignant potential and biology in the liver is unknown, however given their benign behavior in other organs, resection was considered curative.

{kind=link}
{kind=link}