





Abstract
The existing minimally invasive extraction methods for broken intramedullary nails have low success rates. This paper describes the case of a broken intramedullary nail retained distal to the tibia for 12 years, which was removed using a homemade minimally invasive broken nail extractor. We conclude that the homemade minimally invasive broken nail extractor is an effective alternative for removing broken intramedullary nails.
INTRODUCTION
The incidence of nonunion or delayed union of long bone fractures after intramedullary nailing is 15%–20% [1–3]. When nonunion or delayed union occurs, the intramedullary nail is subjected to great stress due to cyclic loading at the fracture level, which can cause fatigue failure of the nail; thus, the breakage of intramedullary nails is not uncommon. Multiple techniques have been described to extract a distal broken piece of nail. Nevertheless, minimally invasive extraction of broken intramedullary nails has a low success rate [4, 5]. This report describes the case of a broken intramedullary nail retained distal to the tibia for 12 years, which was removed using a homemade minimally invasive broken nail extractor.

Preoperative X-ray films showing union of the right tibial fracture associated with a broken intramedullary nail remaining distal to the tibia.
CASE REPORT
A 48-year-old male patient was admitted for requesting removal of all internal implants in his body. He had a closed tibial shaft fracture caused by a collision 15 years prior and was treated with close reduction and intramedullary nailing fixation. Delayed healing occurred after the operation. A nail was broken at a distal locking screw hole. The fracture healed after plaster fixation for 3 months. The internal implant was removed 3 years after the fracture, but the distal end of the broken intramedullary nail could not be removed by the hook removal method and remained in the medullary cavity (Fig. 1). Both operations were performed in another hospital. One year prior to admission, the patient underwent open reduction and internal fixation in our hospital due to a fracture of the right distal radius, and the fracture healed after the operation. His function in the lower and upper limbs recovered well. It can be seen from the preoperative X-ray film that the remaining intramedullary nail was hollow; through measurement, it was known that the outer diameter of the broken nail was 10 mm, which was larger than the isthmus of the medullary cavity.
A minimally invasive broken nail extractor for cannulated intramedullary nails was fabricated, comprising a guide needle and a spear. The diameter of the guide needle was 2.5 mm. The spear contained two 1.0-mm-diameter Kirschner wires with a 2.5-mm-long barb on one side. It was made of medical stainless steel and could be sterilized and reused. The diameter of the barb could be adjusted (Fig. 2).
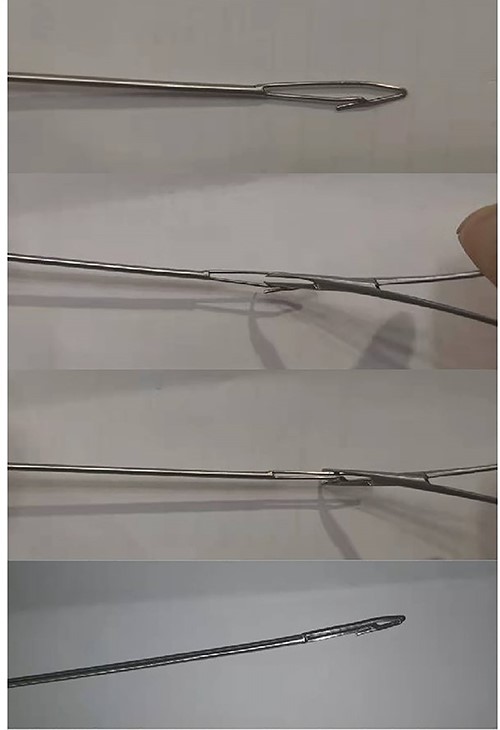
Appearance of a minimally invasive broken nail extractor. The diameter of the spear at the barb could be reduced or expanded.
For the removal procedure, we made a hole at the entry point of the tibia for the intramedullary nail, inserted the guide needle and reamed the tibial medullary cavity with a Φ 11 mm drill bit along the guide needle (Fig. 3). The residue was flushed and aspirated after reaming. We adjusted the diameter of the barb on the spear of the homemade minimally invasive broken nail extractor to 3 mm, then inserted it into the medullary cavity and passed the nail extractor through the canal of the broken nail (Fig. 4). When the extractor was pulled back, the barb hooked the canal wall (Fig. 5) and successfully extracted the broken nail (Fig. 6). The operation was performed under fluoroscopy.

Intraoperative X-ray showing a drill used along a guide needle to ream the medullary cavity.

Intraoperative X-ray showing that the broken nail extractor was inserted into the medullary cavity and passed through the canal of the broken nail.

Intraoperative X-ray showing that the broken nail extractor was pulled back and the barb hooked the canal wall.

The broken nail extractor extracted the broken nail.
DISCUSSION
The existing minimally invasive extraction methods for broken intramedullary nails are the interference fit guide wire method and the hook removal method [6–9]. The interference fit guide wire method entails passing a ball-tipped guide wire and a nontipped guide wire or Kirschner wire through the nail canal, filling the canal as much as possible, and extracting the broken nail using the resistance generated by the friction between the enlarged ball at the front of the wire and the canal wall [6, 7]. The disadvantage of this method is that it is very difficult for the nontipped guide wire and the Kirschner wire to pass through the canal of the broken nail along with the ball-tipped wire. The hook extraction method involves hooking a guide wire through the broken nail canal and extracting the broken nail. The disadvantage of the hook method is that it is very difficult for the hooked guide wire to pass through the broken nail canal. Therefore, both methods have a low success rate.
Our technique is not only simple to manufacture but also reasonable in design. The tip of the extractor is relatively small and is located in the center of the extractor so that it can easily enter the canal of the broken nail and guide the wide barb into the canal. The diameter of the barb can be reduced and expanded. After compression, the barb diameter was ≤3 mm, allowing the body to pass smoothly through the canal of the broken nail. After passing through the canal, the barb diameter was expanded to more than 3 mm, and the barb could easily hook the canal wall of the broken nail. The width of the barb was increased by ~2 mm after full expansion and had exactly the same thickness as the canal wall of the broken nail; thus, it could not hook the medullary cavity wall and become stuck. The diameter of the barb was 1.0 mm and had a certain resistance to bending, allowing the broken nail to be extracted even if there was some resistance.
The main points of the operation are as follows: When the broken nail extractor is expected to encounter great resistance through the medullary cavity, especially the isthmus, the medullary cavity must be reamed with a drill; otherwise, the barb will be broken or bent. Second, the diameter of the barb should be adjusted according to the inner diameter of the broken nail; if it is too small, the barb will not easily hook the canal wall of the broken nail when it is pulled out; if it is too large, it will be difficult for the barb to pass through the canal of the broken nail. Therefore, it is best to be consistent with or slightly larger than the inner diameter of the broken nail.
We used a minimally invasive broken nail extractor to remove a broken intramedullary nail remaining in the distal end of the medullary cavity on cadaver specimens, and the removal rate was 100%. This is the first case of the successful removal of a broken intramedullary nail remaining in the distal tibia using this method, whereas other minimally invasive removal methods have failed, indicating that the homemade minimally invasive broken nail extractor is an effective alternative for removing broken intramedullary nails.
AUTHORS’ CONTRIBUTIONS
C.W., J.L. and Q.Y. conceived the study. C.W., G.M. and Y.L. drafted the manuscript. S.G. performed the literature search. G.M. contributed to the clinical management of the patient. Q.Y. and G.M. performed the surgery of this patient. Q.Y. and J.L. revised the manuscript critically and approved the modified text. All authors read and approved the final manuscript.
ACKNOWLEDGEMENTS
The authors would like to express their gratitude to AJE (https://www.aje.com/) for the expert linguistic services provided.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
Funding for this project was provided by the top medical expert team of ‘The Taihu Talent Program’ in Wuxi (2020) (TTP-2020100), the ‘Innovation and Entrepreneurship Program for Excellent Doctorate’ of Wuxi No. 9 People’s Hospital (WX9PH-IEPED-02) and the ‘Wuxi Science and Technology Development Fund Project’ (2022) (WXSTDFP-2022-05).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}