





Abstract
Partial nephrectomy has been established as a standard treatment of renal mass <4 cm(cT1a), but mostly it is performed in larger tumors of size up to 7 cm (cT2b). The maximum size of a tumor that could undergo partial nephrectomy is controversial. In this case report, we present a case of a large renal mass (17 cm) that underwent open partial nephrectomy successfully. To our knowledge, this case is the giant tumor that underwent partial nephrectomy in the literature. Partial nephrectomy could be performed if technically feasible irrespective of the tumor size.
INTRODUCTION
Partial nephrectomy has been established as a standard treatment of renal mass <4 cm(cT1a), but mostly it is performed in larger tumors of size up to 7 cm (cT2b) [1]. With the increase in comorbidities such as hypertension and diabetes mellitus, the indications for partial nephrectomy are evolving, especially in more significant and complex tumors. The different surgical approaches (open, laparoscopic and robotic) for renal mass have similar surgical and oncological outcomes [1, 2]. The maximum size of a tumor that could undergo partial nephrectomy is controversial. This case report presents a large renal mass (17 cm) that successfully underwent open partial nephrectomy. To our knowledge, this case is the giant tumor that underwent partial nephrectomy in the literature. In our case, the main reason for partial nephrectomy was the familial history of bilateral renal tumor and the patient’s concern regarding contralateral tumor occurrence. The patient followed up as standard protocols; the follow-up imaging studies revealed normal-appearing renal anatomy without recurrence.
CASE PRESENTATION
A 22-year-old man was referred to our clinic with ambiguous abdominal pain radiating to the left flank. The patient had a history of diabetes mellitus from 3 years ago. Also, he had a familial history of renal failure due to bilateral renal mass resection in his father. The physical examination revealed a left flank mass. The laboratory tests, including renal function and liver tests, were routine except for microscopic hematuria. In contrast-enhanced abdominal computed tomography scan, huge left renal mass with contrast enhancement was a noticeable finding (Fig. 1). The patient was scheduled for radical nephrectomy, but due to the family’s history of bilateral renal tumor and concern of patients regarding contralateral tumors in the future, he refused to undergo radical nephrectomy. Due to the size of the tumor, we choose to perform open surgery. The operation was performed through a flank incision in the bed of the 12th rib. Despite the large tumor size, we approached the tumor extraperitoneal. During the surgery, we encountered a vast left renal mass. Initially, we released the ureter to avoid accidental injury, then obtained early access to the renal pedicle to control bleeding with a Satinsky clamp.
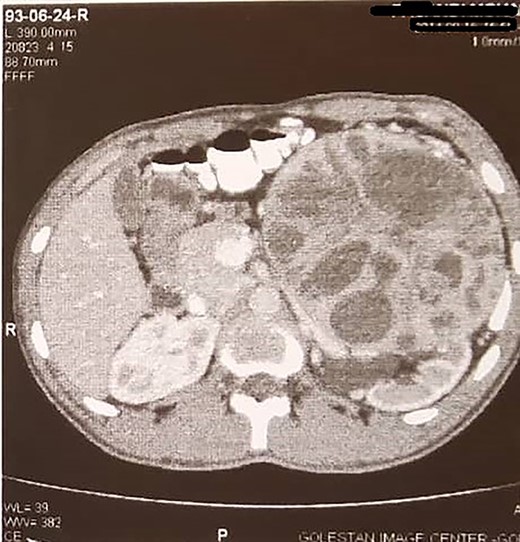
Large left renal mass.
Surprisingly the mass enucleated without any difficulty and was removed uneventfully (Fig. 2). The warm ischemic time (WIT) was 30 min. A good rim of the normal kidney remained after mass resection. The renal defect was repaired with 4/0 vicryl on multiple rolls of surgical that anchored to the renal defect. In the follow-up, the renal function test was regular (Cr:1.2). The patient was discharged postoperative on the third day without any complications. The surgical pathology reported the solid-cystic mass (17 × 16 × 9 cm) as renal cell carcinoma (conventional type) with Fuhrman grade 2 and negative surgical margin. We followed up with the patient after surgery according to the standard imaging protocol in partial nephrectomy cases. Figure 3 depicts the last follow-up of the patient 7 years after surgery.
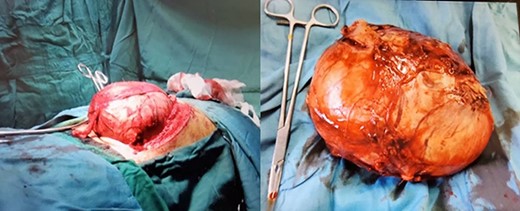
Huge renal mass during surgery and removed mass.

The follow-up image revealed normal-appearing left kidney.
DISCUSSION
Nowadays, partial nephrectomy is an accepted modality of choice in treating renal mass up to 7 cm (cT1b), with similar oncological and functional endpoint outcomes compared with radical nephrectomy. Recent studies have confirmed the role of partial nephrectomy in tumors with larger size (cT2), although the risk of impaired renal function and complications will be increased as the size of the tumor increases [3]. A study by Breau et al. [4] confirmed the feasibility of partial nephrectomy in cT2 and larger renal tumors with better preservation of the renal function.
Although many experts recommended laparoscopic partial nephrectomy in the management of renal mass in patients with predisposing factors to chronic kidney disease, bilateral tumors and tumors in a single kidney in some situations like our case with a large size tumor, in more complex tumors such as central or endophytic tumors and reoperation surgery the open partial nephrectomy is a more helpful modality with comparable functional and oncological outcomes [2]. The postoperative complications will increase as the size of the tumor increases, but the main concerns regarding performing partial nephrectomy in larger tumors are the oncological outcome. The recent reports mentioned that although the complication rate is higher in larger tumors, recurrence and survival are not significantly different between partial and radical nephrectomy groups [5].
In our case, we encountered a patient with a huge left renal mass and a history of diabetes mellitus from 3 years ago and of bilateral renal tumor in his father, but due to the large size of the tumor, he candidate to undergo open radical surgery. We found the tumor encapsulated and easily enucleated during the surgery despite its size. To our knowledge, this case is a giant tumor that underwent partial nephrectomy without significant complication. The follow-up laboratory tests and imaging study revealed normal findings, so it seems that in such patients, we could consider partial nephrectomy if feasible.
CONCLUSIONS
In patients with renal mass that have an underlying risk factor for chronic kidney disease or familial history of bilateral renal mass, partial nephrectomy could be performed if it is technically feasible irrespective of the tumor size.
AUTHOR’S CONTRIBUTIONS
S.M.K.A. carried out investigation and manuscript writing—original draft. A.M. worked on investigation and manuscript writing—review and editing, supervision.
ACKNOWLEDGMENT
The authors would like to thank the patient, the Urology research center at Sina hospital.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}