





Abstract
Neimeier, in 1934, proposed a classification for gallbladder perforation. The first type is fistulation between the gallbladder and adjacent viscerae. The second type is a subacute perforation surrounded by an abscess walled off by adhesions from the general peritoneal cavity; and the third type is a peritonitis due to free biliary spillage into the peritoneal cavity without protective adhesions. We will analyze a Neimeier’s type 1 perforation. The patient is a 72-year-old male diagnosed with a cholecystolithiasis and empyema due to a cholecystopleural fistula. Was operated by laparoscopic surgery because its low rate of complications, and lower days at hospital staying. Everything went as planned with no complications. Even though it is not a common presentation, it sets a precedent for it to be furthermore researched, and for it to be used as a literary option in a discussion to know which type of surgery is better for these cases.
INTRODUCTION
Biliary fistulas are not frequent, only between 1% and 3% of patients with stones inside the bile ducts may develop a type of biliary fistula [1]. Biliopleural fistulas are rare cases with a very varied etiology (infectious, iatrogenic, traumatic, congenital or obstructive). This type of pathology is divided into four main categories: acquired (infectious process and iatrogenic injuries), traumatic (open trauma or closed trauma), congenital (malformations of the biliary tree) or obstructive (neoplasia or gallstones) [1]. The suspicion of this pathology must be clinical, and it must be confirmed with advanced imaging evidence. Diagnostic methods in this pathology may be computed axial tomography, nuclear magnetic resonance, bile duct ultrasound, percutaneous cholangiography and diagnostic endoscopy (ERCP) [1, 2]. As biliar fistulas are not a frequent problem, there is not enough information (worldwide and in Mexico) about them, and the surgical techniques used to solve them. Therefore, the purpose of this paper is to expand the information related to this topic and present an interesting case and the surgical management.
CASE REPORT
A 72-year-old male with a history of no previous operations or traumas, with diabetes mellitus, systemic arterial hypertension, dyslipidemia, hypothyroidism, chronic kidney disease and chronic obstructive pulmonary disease with a diagnosis of uncomplicated cholecystolithiasis in 2015. The condition began 7 days prior to admission with intermittent colicky pain in the right upper quadrant accompanied by nausea and vomiting. He was admitted to the emergency room after referring pleuritic chest pain in the right hemithorax as well as dyspnea of medium efforts. The patient undergoes an immediate chest x-ray finding pleural effusion, as well as general laboratory studies are made. Laboratory results reported a hemoglobin of 12.2 g/dl, hematocrit 38.1%, white blood cells count 25 K/μl, neutrophils 69.4%, total bilirrubin 0.7 mg/dl, and direct bilirubin 0.2 mg/dl.
A thoracentesis was performed in the right hemithorax with an outflow of 1000 cc of cloudy, nonfetid yellow pleural fluid with Light criteria for exudate. Therefore, pleural tube placement is considered in the patient. Pathology reports the fluid drained had a pH of 8.5, white blood cell count of 470 cu/mm3 with 67% polymorphonuclear cells, total bilirrubin 4.2 mg/dl, and direct bilirrubin 1.1 md/dl. A contrasted chest tomography (Fig. 1A–C) was performed with an extension to the upper abdomen, where a perforated cholecystolithiasis was reported with a probable cholecystopleural fistula forming an empyema with a volume of 3244 cc. A right chest tube was placed, and a laparoscopic cholecystectomy was scheduled plus closure of the cholecystopleural fistula. Later, the gallbladder was sent to the department of pathology to rule out any probable cancer, obtaining a negative result for neoplasia.

(A) Cholecystopleural fistula by contrast-enhanced thoracic CT. (B) Axial view that shows the perforation of the funds of the gallbladder with disruption of the right hemidiaphragm. (C) Coronal view that shows the perforation of the funds of the gallbladder with disruption of the right hemidiaphragm.
Surgical technique
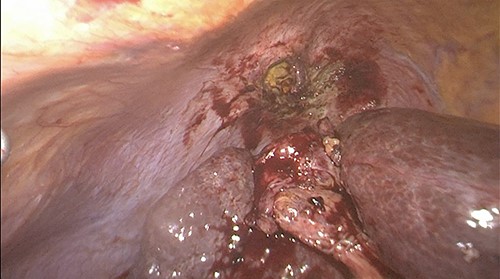
Prior to the surgical protocol, prophylactic antibiotics (ceftriaxone 1 g and metronidazole 500 mg) were administered during anesthetic induction. Three trocars were placed to perform the surgical procedure, one 11 mm supraumbilical (optical) and two 5 mm in the epigastrium and in the right upper quadrant. Pneumoperitoneum was induced with closed technique and the patient was placed in the reverse Trendelenburg position to begin the procedure. Inside the abdominal cavity, we observed the gallbladder adhered to the diaphragm (Fig. 2). The gallbladder was dissected, leaving the fundus of the gallbladder attached to the diaphragm (Fig. 3), the pleura and its movements were not appreciated, and lung tissue was not identified through the orifice. We could see a thick inflammatory tissue sealing the defect. Two giant stones were removed from the gallbladder’s fundus (Fig. 4) and the gallbladder was dissected antegrade. Cystic artery and duct were identified using Strasberg’s critical view of safety (Fig. 5). One distal and two proximal staples were placed in the cystic duct and cut, as well as a distal and one proximal staple in the cystic artery to cut as well. Later the gallbladder and stones were removed. Before ending the procedure, a drain was placed into the surgical wound, hemostasis was checked, and trocars were removed under direct vision. Finally, the fascia was closed with a 1–0 absorbable suture and the skin is closed with a 4–0 suture. There was no complications nor side effects in the mediate and immediate postoperatory.

Gallbladder adhered to the diaphragm.
Fundus of the gallbladder adhered to the diaphragm after dissection.
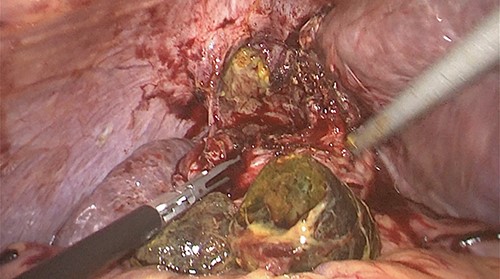
Two stones removed from the fundus.
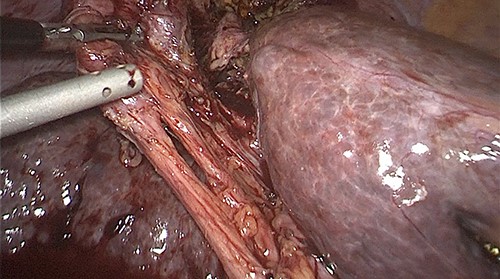
Cystic artery and cystic duct identified by using Strasberg’s critical view of safety.
Follow-up and outcomes
The patient was discharged 10 days after the surgery with no complications and the follow-up was made a week after at the hospital and it was uneventful. The short-term postsurgery indications were resting, and after the first 24 hours the patient started to move. There was no specific long-term surveillance requirement.
DISCUSSION
Biliary fistulas are a rare pathology, present in 10% of gallbladder lithiasis [3]. These fistulas can drain in several parts of the body, such as: liver, duodenum, jejunum, ileum, stomach, colon, lungs and even through the skin. As compared with different literature, the main strength of this case report is the innovation it provides for the management for this pathology using laparoscopic surgery in the country. Almost each one of these case reports, used laparoscopic surgery as treatment for this. Laparoscopy is considered as the main treatment for this pathology because it gives good results with lower rates of complications and reduces the time of staying at the hospital [4]. Other treatments as endoscopic retrograde cholangiopancreatography with a sphincterotomy (in the sphincter of Oddi) has been used to solve this problem, showing good improvement for the patient [5, 6]. If this does not work, laparoscopic surgery is indicated.
For the diagnosis of this pathology, an enhanced thoracic computed tomography (CT) scan is the gold standard. In comparison, it has higher sensitivity against ultrasound (92% vs. 79%). Also, one of the advantages of the CT scan, is helping the surgical team an adequate planning of the surgery.
In the research to make this case report, it was found that thoracoabdominal trauma can cause cholecystopleural fistulation; specifically, the open wounds caused by gunshots or stabbing [5, 7, 8]. This can be an important outcome in case that a patient with an open wound starts with symptoms like colicky pain in right upper quadrant, nausea, dyspnea, pleuritic chest pain, etc. According to the results shared by the reports that were consulted, almost all of them conclude to say that minimal invasive surgery represents the gold standard. The only disadvantages are that they must be performed by someone specialized and the cost for the patient could increase; but the advantages are bigger and better than the disadvantages [9].
Finally, is important to know if this changes in some other patient with some different conditions and know how and why it changed the result, so we exhort other surgical teams to go further with the research about this topic [10].
ACKNOWLEDGMENT
Universidad Autónoma de Nuevo León, Hospital Universitario ‘Dr. José Eleuterio González’, Department of General Surgery, Monterrey, Nuevo Leon, Mexico.
CONFLICT OF INTEREST STATEMENT
None declared.
INFORMED CONSENT
We have the permission of the patient to report this case.
GUARANTOR
Manuel de la O is acting as a guarantor of the case report.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}