





Abstract
Papillary carcinoma originating from a thyroglossal cyst represents an infrequent finding, which occurs in ~1% of cases of thyroglossal cyst and its presentation is usually the same as that of a benign cyst, which represents the most frequent benign congenital lesion of the neck. The diagnosis is usually presented as a finding on the histopathological examination. Two cases of a thyroglossal cyst with later development of malignancy are presented. The first, a 30-year-old female, and the second, a 32-year-old male. Both began their condition after presenting an increase in volume in the neck, the female presented a right sub-mental triangle of 1 year of evolution, and the male on the anterior side of the neck. In both cases, the diagnosis of thyroglossal cyst was made by the physical examination and findings of cervical ultrasound and computed axial tomography. Surgical management consisted of the Sistrunk procedure with a definitive histopathological result for papillary thyroid carcinoma originating from thyroglossal cyst. In the case of the male patient, the Sistrunk procedure was performed along a total thyroidectomy, although in the female patient, a total thyroidectomy was performed in a second stage. Patients were then discharged and referred to the endocrinology service for further medical treatment. The management of these cases continues to be controversial due to the limited number of reported cases, so the multidisciplinary management and individualization of each case plays a fundamental role in the management of this rare condition.
INTRODUCTION
From the embryological point of view, the thyroid gland develops from an invagination of the midline of endoderm cells, between the third and fourth week of embryological development, this epithelial invagination descends from the base of the tongue along the midline towards the anterior section of the neck towards the first and second tracheal rings [1]. The hyoid bone develops in the mesoderm of the second and third arch, so that the thyroglossal tract passes ventral to it. The thyroglossal duct obliterates its path between the 8th and 10th week of gestation, the failure to obliterate some portion of this canal produces a cystic defect known as a thyroglossal cyst, which is estimated to be present in 7% of the general population [2]. The thyroglossal duct cyst arises as a cystic expansion of a remnant of the thyroglossal duct tract. The stimulus for expansion is not well known, but the lymphoid tissue associated with the duct tract is thought to hypertrophy at the time of regional infection, occluding the tract resulting in cyst formation [3]. Many thyroglossal cysts are never clinically detected. A postmortem study conducted in 1976 in Toronto, Canada studied 200 adults where an incidence of 7% of thyroglossal duct cysts was found [4]. Rarely, malignancy from a thyroglossal cyst may develop with an incidence of <1%. Most of these carcinomas are of the papillary type with a presentation similar to that of the thyroglossal cyst [5].
CASE SERIES
Case 1
A 30-year-old female with no pathological personal history began on august of 2016 with an increase in volume in the right sub-mental triangle of 1 year of evolution (Fig. 1). The diagnosis of thyroglossal cyst was made 1 year later by the physical examination and findings of cervical ultrasound and computed axial tomography, which were compatible with a malignant lesion, reason for which a histopathological study was requested by ultrasound guided fine-needle aspiration biopsy. A 75 mCi I 131 thyroid scintigraphy was performed with normal uptake, 16% in the usual situation of the thyroid with preserved shape and function (Fig. 2).

Clinical image of the lesion during physical examination.
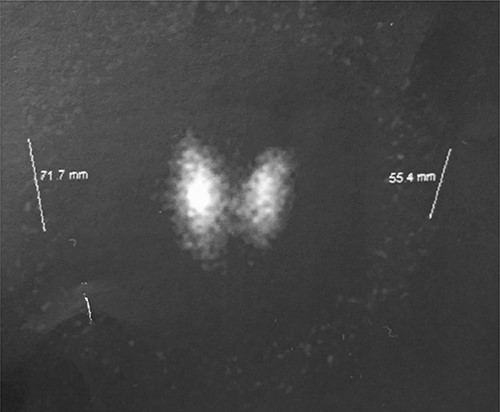
Thyroid gram range 75 mCi I 131 with normal uptake 16% in normal thyroid situation with preserved shape and function.
The patient underwent surgical management 2 weeks later with wide resection of the lesion including the affected hyoid bone segment, with a definitive histopathological result for papillary thyroid carcinoma originating from the thyroglossal cyst (Figs 3 and 4). Following the algorithm of treatment, a total thyroidectomy was performed in a second stage. Subsequently, the management was supplemented with radioactive iodine therapy and thyroid supplementation.
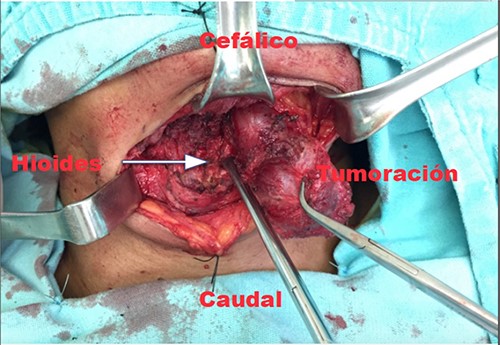
Intraoperative exposure of the right cervicotomy of the hyoid bone in relation to the tumor (arrow).

In bloc resection of thyroglossal cyst including hyoid bone segment.
Currently, our patient is under an adequate thyroid supplementation treatment, free of disease and under follow-up at our institution.
Case 2
Following the first case, a case of a 32-year-old male presented in our consult. The patient had a smoking history of 2–3 daily tobacco cigarettes for 10 years, and alcoholism; childhood relevant history showed that the patient was born prematurely. The familiar history revealed a mother with hyperthyroidism, and a grandfather with hyperthyroidism with iodine treatment.
Two months ago, the patient began with a volume increasing mass in the anterior side of the neck, without any added symptoms. The patient visited a physician who asked for a thyroid ultrasound, which was performed on august 16th of the present year. The study showed a midline-neck heterogeneous cystic mass. The follow-up plan included a contrast-enhanced computer tomography scan, to analyze the possibility of a neo proliferative mass, as the radiology specialist suggested. The scan was performed 2 days later, and it revealed a solid cystic tumor, with multiple septa, localized on the midline adjacent to the thyroid gland and its pyramidal lobe (Fig. 5). The histopathology report suggested a thyroglossal duct cyst related to a papillary-type thyroid cancer (Fig. 6).
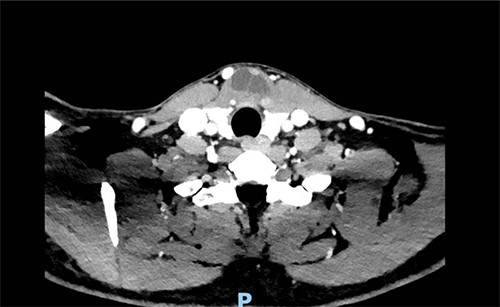
Solid cystic tumor, with multiple septa, localized on the midline adjacent to the thyroid gland.
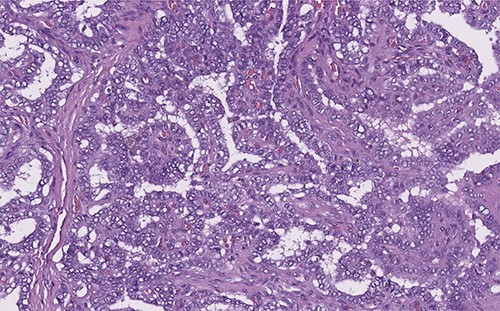
Papillary thyroid carcinoma: true papillae with multiple branching, stromal stalk with microvessels (left). Note the optically clear (empty, ground-glass) nuclei with thick nuclear membrane (H&E, high power).
On 24 August 2021, an ultrasound guided fine-needle aspiration biopsy was performed on the thyroglossal duct cyst. The liquid content of the cyst was then analyzed with cytology and revealed a thyroid papillary carcinoma.
The patient was then referred to an oncologist surgeon for further analysis, who decided to perform a Sistrunk and total thyroidectomy procedure (Figs 7 and 8). The surgery was performed on the 1 October 2021 without complications on the postoperative follow-up. The patient was then discharged and referred to an endocrinologist for further follow-up.
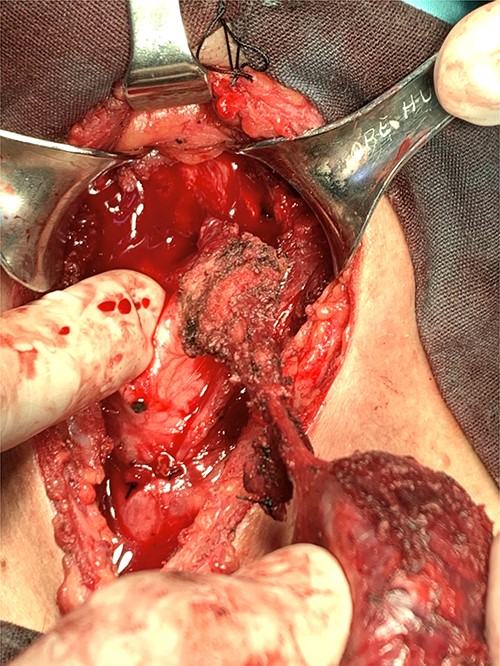
Removing the thyroglossal duct cyst carcinoma.

Thyroglossal duct cyst related to a papillary-type thyroid cancer.
DISCUSSION
Papillary carcinoma originating from a thyroglossal cyst represents an infrequent finding, which occurs in approximately 1% of thyroglossal cyst cases. Papillary thyroid cancer is reported in 85–91% of cancer cases associated with thyroglossal cyst, followed by mixed, follicular and squamous papillary. Its presentation is usually the same as that of a benign cyst, which represents the most frequent benign congenital lesion of the neck. This type of cancer is more common in adults with a 2.3:1 female:male ratio. The main symptom at the beginning is a mass in the cervical region, however, they may present dysphagia or hoarseness [6]. A study carried out from the database of the pathology department between 2005 and 2015 that included 12 patients with this type of cancer, fine needle aspiration (FNA) biopsy was practiced. The FNA had a 53% true positive rate and a 47% false negative rate. This lack of efficacy has been largely attributed to low cellular yield secondary to the cystic nature of the lesion and the relatively small size of the malignant component [7]. The diagnosis is usually presented as a finding on histopathological examination [1].
Regarding the pathogenesis of this entity, two theories have been proposed for its origin. It develops as a direct metastasis of a papillary thyroid carcinoma or is generated de novo from ectopic thyroid tissue located in the cyst, which is reported to be present in up to 62% of the pieces of pathology obtained [3].
Since both pathologies present clinically in a very similar way, the diagnosis is usually a finding in the histopathological report. The suspicion of a carcinoma of a thyroglossal cyst can be suspected from the affection of the surrounding tissues, atypical location, firmness of the same or involvement of adjacent structures, risk factors such as radiation, as well as the presence of adenopathies or alterations of the same thyroid gland [8].
Imaging studies such as ultrasound, tomography and nuclear magnetic resonance provide valuable information when findings suggestive of malignancy are found, such as invasion of neighboring structures, calcifications or associated suspicious adenopathies, however, by themselves they do not represent a reliable diagnostic method [9].
The cytological examination obtained by FNA is only diagnostic in 66% of the cases, as reported by Chala et al. [8], with papillary carcinoma in 87% of cases, 5% squamous, 1.7% follicular and 0.9% anaplastic [5, 10].
In most cases, carcinoma originating from a thyroglossal cyst is treated with a resection with the Sistrunk procedure, with a reported 95% cure. In the Sistrunk procedure, the cyst, part of the hyoid bone and the thyroglossal duct are removed all together [6]. Some studies advocate the need for a total thyroidectomy in all patients due to the high risk of an unsuspected infiltration with thyroid involvement of a papillary thyroid carcinoma. Thyroidectomy also allows for further optional radioactive iodine treatment and a more effective use of thyroglobulin levels for surveillance and follow-up [7]. The prognosis is excellent and reported distant metastases are very rare.
CONCLUSION
Thyroglossal duct cyst-associated with carcinoma is usually not suspected preoperatively. The management of these cases continues to be controversial due to the limited number of reported cases, so multidisciplinary management and individualization of each case play a fundamental role in the management of these rare cases.
The clinical presentation in these patients can be highly variable and the clinical suspicion of the presence of a carcinoma derives from the presence of masses with infrequent localization as well as those that are invading adjacent tissues, as well as the presence of lymphadenopathy or alterations of the thyroid gland.
The Sistrunk procedure appears to be adequate for most of the patients, and only in some selected cases is total thyroidectomy or cervical lymph node dissection indicated. The staging of the tumor based on its size, histopathological findings, disease-free borders, age, and the presence of lymphadenopathy or metastasis are factors that will determine the treatment to be followed. The follow-up of these cases is usually the same, followed in papillary thyroid carcinoma, based on clinical judgment and other studies. The prognosis for patients with papillary cancer associated with thyroglossal duct cyst is excellent.
CONFLICT OF INTEREST STATEMENT
There are no conflicts of interest for this publication.
We have the permission of the patients to report both cases, Manuel de la O-Escamilla is acting as a guarantor of the case report.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}