





Abstract
Urethral catheterization is one of the most common procedures in medical practice. Catheterization is not only restricted for urological purposes, but also used for many other indications. For instance, urethral catheterization could be used for intensive care unit patients, trauma and multiple fracture injuries, and advanced neurological condition e.g. multiple sclerosis. Therefore, it may be performed by both well trained and not fully trained medical professionals resulting in complications. We present an 82-year-old female presented to A&E with hematuria, abdominal pain and low catheter output drainage after recent catheter exchange by the district nurse. Interestingly, non-contrast computed tomography (CT) scan showed the catheter inserted into the left ureter and the catheter balloon was inflated at the level of the mid-ureter. Later contrast CT study showed extravasation confirming ureteric wall partial disruption injury. The patient was managed conservatively without apparent complications in the follow-up.
INTRODUCTION
Bacteriuria is a common phenomenon associated with long-term catheter (LTC) placed for more than 10 days [1]. Biofilms, which are a collection of microorganisms mixed with urine proteins, colonize the surface of the catheter. Subsequently, the bacteria are being protected from antibiotic effect. In addition, unjustified antibiotic use might lead to developing more resistant strains [2]. The presence of bacteriuria and chronic infection associated with LTC could lead to mechanical complications as well. For instance, spontaneous bladder rupture could occur in LTC patient [3]. Other factors might make LTC mechanical complications more complex including the poor general health of LTC patients and associated medical comorbidities e.g. diabetes mellitus & multiple sclerosis. In addition, lack of proper medical records, particularly for the elderly patient, could lead to further complications. Urethral catheterization in patients with underlying urological conditions might lead to unexpected urological trauma [4].
CASE PRESENTATION
A frail 82-year-old female presented to the A&E department 24 h after having a urethral catheter exchange by the district nurse. She complained of abdominal pain, low catheter output with bypassing, and mild hematuria.
On examination, the patient was feverish (temp 38.2) and had left sided abdominal pain without tenderness on palpation. Her blood investigations did not show any significant changes. Initial washout through the catheter increased the pain and it showed passive drainage only. Non-contrast computed tomography (CT) was performed to assess the catheter position. Surprisingly, the catheter was passing into the left ureter with the catheter balloon inflated in the mid-ureter (Fig. 1).

Coronal section of abdomen and pelvis non-contrast CT: The urethral catheter migrates into the left ureter up to the mid-ureter.
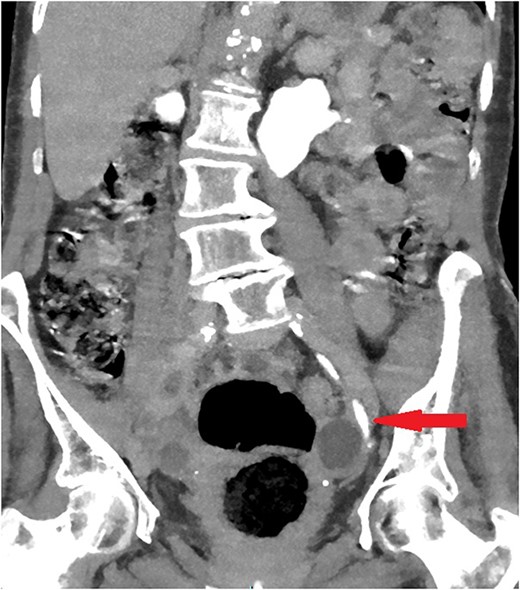
The old catheter was removed, and a replacement was inserted correctly into the bladder. The patient was managed conservatively with antibiotics. A further contrast CT was performed and showed mild extravasation of the contrast at the same level of the former catheter’s inflated balloon (Fig. 2). The patient improved clinically with conservative management, and her blood investigations remained stable. Follow-up contrast CT after 2 months was normal and showed no extravasation and no stricture (Fig. 3).
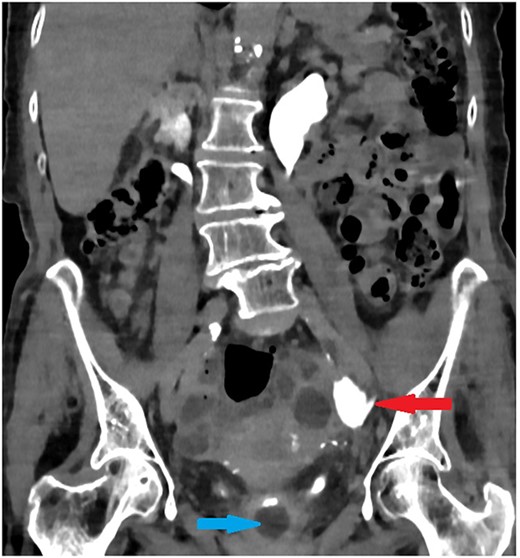
Coronal section of abdomen and pelvis contrast CT 24 h from the initial CT: The new urethral catheter balloon in the bladder (blue arrow). Contrast extravasates the left ureter at the site of the old catheter balloon (red arrow).
Coronal section of abdomen and pelvis contrast CT 2 weeks after the injury: Contrast flows normally without extravasation or stricture in the left ureter.
DISCUSSION
Urosepsis is a medical emergency and represents almost 30% of total cases of sepsis, with mortality rate 30–40% [5]. LTC is almost always associated with chronic bacteriuria. Therefore, any LTC related complications could lead to significant morbidity or even mortality.
Desai et al. reported one case of ureteric injury caused by LTC in male patient with bilateral vesico-ureteric reflux (VUR) grade 4 [6]. The case has similar presentation and was managed conservatively as well. They reported low sensitivity of the ultrasound and highlighted the importance of CT in accurate diagnosis.
Luo et al. published a review included 23 cases of urethral catheter inadvertently placed into the ureter, 5 cases were caused by supra-pubic catheter [7]. Only three cases (13%) needed surgical repair (Fig. 4). Most of these cases had LTC secondary to neurogenic bladder, with female predominance (3:1). LTC might lead to contracted bladder, facilitating LTC to pass into the ureter in the presence of VUR. In addition, the short urethra in female might increase the risk of ureteric placement of LTC.
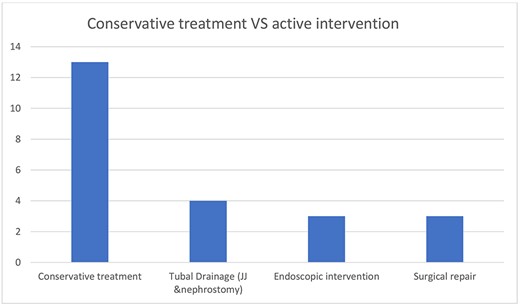
Luo et al. review: Only three cases (~13%) needed surgical repair. Three cases needed endoscopic deflation of the catheter balloon. Four cases needed urinary diversion, three with JJ ureteric stent and one with nephrostomy due to failed ureteric stenting. Thirteen cases were treated conservatively with simple catheter replacement.
Similarly, our case presented with urosepsis, inadequate catheter drainage and abdominal pain, which increased with washout. Early diagnosis with CT contributed to the management outcome. Interestingly after reviewing the patient records, the patient was diagnosed with VUR 20 years back. However, it was not reported by neither the patient nor accompanied carers at the time of the incident.
History-taking in an elderly patient might be difficult because of many factors including age related cognitive dysfunction and hearing difficulty [8].
Therefore, it would be of high importance to report the underlying urological conditions for the patients using a LTC in their medical records and catheter passports. For instance, VUR and previous major bladder surgery could lead to direct mechanical complications with major impact including urosepsis, need for surgical management and increase of burden on health care system [4, 7].
CONCLUSION
In patients with LTC, underlying urological conditions should be reported clearly in their catheter passport, particularly if causing anatomical impact. Abnormal or reduced urine output, fever, and abdominal pain should increase the awareness of catheter related complications. CT scan should be the initial imaging modality for assessment because it would lead to early diagnosis. Subsequently, it would increase the chance of conservative treatment with a better outcome.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}