





Abstract
Colorectal cancer represents the third most common cancer worldwide. The presence of peritoneal metastasis of colorectal cancer indicates Stage 4 disease with poor prognosis. We report a case of a foreign body reaction to plant material spilled during previous surgery, which mimicked peritoneal metastases. A 62-year-old male was found to have recto-sigmoid adenocarcinoma on colonoscopy. At the time of resection, peritoneal nodules were identified throughout the peritoneal cavity with the appearance of metastases. The resection was aborted, a diverting colostomy was fashioned and biopsies of the nodules were taken. The histology showed a foreign body reaction to plant material that was spilled during a sleeve gastrectomy that was performed 4 years prior. The patient subsequently underwent anterior resection with anastomosis and has recovered from surgery.
INTRODUCTION
Colorectal cancer is the third most common cancer worldwide, with ~945 000 new cases yearly [1]. The mainstay of curative treatment is surgical resection, however, the prognosis depends on the stage of disease. The presence of peritoneal carcinomatosis indicates TNM Stage 4 disease with 0–7% 5-year survival [1]. Peritoneal carcinomatosis is encountered in ~7% of patients at the time of primary resection [2]. Treatment options include cytoreductive surgery and hyperthermic intraperitoneal chemotherapy [1].
Approximately, 252 000 bariatric procedures are performed each year in the USA alone. Sleeve gastrectomy represents 61% of these [3]. Staple line leakage is the most dangerous complication of sleeve gastrectomy and occurs with an incidence of 2.1% [4, 5]. There are no reported cases of gastric contents being spilled during the procedure, however, this can occur in practice.
We present an unusual case in which a foreign body reaction to plant material spilled during previous sleeve gastrectomy had the intra-operative appearance of peritoneal metastatic lesions.
CASE REPORT
A 62-year-old male underwent a colonoscopy to investigate anaemia and positive faecal occult blood tests. This identified a 4-cm adenocarcinoma at the rectosigmoid junction. Staging imaging, including computed tomography (CT) chest/abdomen/pelvis, magnetic resonance liver and FDG positron emission tomography (PET) scan, showed only a solitary segment 8 hepatic lesion which was highly suspicious for metastasis. After multi-disciplinary team discussion, the patient was booked for laparoscopic anterior resection with a plan for subsequent chemotherapy and then resection of the hepatic metastasis.
The patient’s medical history included Type 2 diabetes, hypertension, asthma and a sleeve gastrectomy 4 years prior for obesity. The sleeve gastrectomy was performed at another institution and was complicated by a spill of gastric contents during the procedure. It is unclear what measures were taken to decontaminate the abdomen at the time.
Upon laparoscopy, multiple peritoneal nodules with the appearance of metastatic disease were observed throughout the abdomen (Fig. 1). These nodules were seen in the right upper quadrant, right flank and in the pelvis fusing the recto-sigmoid colon to the anterior abdominal wall. The largest lesion measured 2 × 3 cm. The resection was aborted, a diverting colostomy was fashioned proximal to the cancer and biopsies of peritoneal nodules were taken.
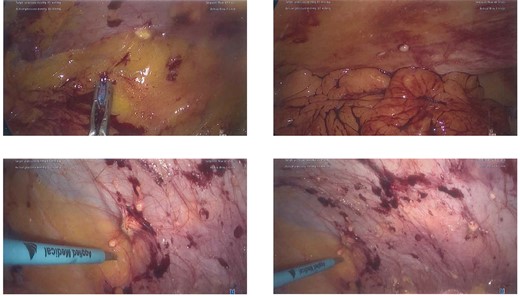
Intra-operative photographs of peritoneal nodules.
The histology of the biopsies showed a florid foreign body giant cell and histiocytic reaction to extensive vegetable material. No evidence of malignancy was identified. Given the benign nature of the lesions, the patient subsequently underwent anterior resection with anastomosis as previously planned. The histology showed T3N1b adenocarcinoma of no special type. The patient has recovered from surgery and is currently completing chemotherapy.
DISCUSSION
The peritoneal nodules identified in this case represented a reaction to plant material spilled during sleeve gastrectomy, which had been retained within the abdomen for 4 years. There are only limited other cases of intra-peritoneal foreign body reactions mimicking metastases reported in the literature.
Akita et al. reported a case of spontaneous gastric perforation which was repaired surgically. Subsequent endoscopy identified gastric adenocarcinoma. At the time of surgery to resect the cancer, small peritoneal nodules were identified, which were thought to represent metastases. Frozen section specimens were taken, which did not identify carcinoma, then a distal gastrectomy was performed. The formal histology of the peritoneal nodules revealed foreign body granulomas [6].
In a related article, Kim et al. reported a series of three patients who were treated with intra-peritoneal chemotherapy at the time of surgery for advanced gastric cancer with no known metastases. On surveillance CT scans 6 months post-operatively, peritoneal lesions were identified in all three patients. These lesions were avid on FDG PET. One patient proceeded to diagnostic laparoscopy which identified black coloured nodules throughout the peritoneal cavity. Histology showed foreign body granulomas with extensive carbon deposits. This was consistent with a reaction to activated charcoal that was included in the intra-peritoneal chemotherapy to prolong high concentrations of the chemotherapy agent within the peritoneal cavity [7].
Foreign body reaction should be considered as a differential diagnosis in patients with peritoneal nodules who have had previous gastrointestinal perforation/leak. The presence of peritoneal metastasis in colorectal cancer has a significant impact on prognosis and treatment. This case reinforces the importance of taking biopsies to confirm the diagnosis when peritoneal nodules are encountered.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}