





Abstract
Minimally invasive surgery for large thymic malignant tumors remains challenging. Here, we demonstrate dual-scopic robotic thymectomy for a challenging malignant thymic tumor. An asymptomatic 70-year-old woman clinically diagnosed with a large thymic malignant tumor invading the left phrenic nerve and pericardium underwent surgery. After dissecting the left phrenic nerve and pericardium under left unilateral video-assisted thoracic surgery, a robotic subxiphoid approach was conducted to achieve complete thymectomy. During robotic surgery, the large tumor sometimes limited the surgical view. To overcome this limitation, we added a conventional thoracoscope and utilized both images of the conventional thoracoscopic view and robotic camera via TilePro display to achieve complete resection of the thymic epithelial tumor. The patient was discharged with no complications except left phrenic palsy. The pathological diagnosis was a thymic neuroendocrine tumor invading the left phrenic nerve. This approach is potentially useful in surgery for challenging thymic malignant tumors.
INTRODUCTION
Minimally invasive surgery for large thymic malignant tumors remains challenging even under robotic thoracic surgery. We herein present a ‘dual-scopic’ robotic thymectomy using images from both a robotic camera and a conventional thoracoscope to achieve safe and complete resection of a challenging thymic malignant tumor.
CASE REPORT
A 70-year-old woman with no symptoms was referred to our hospital because of an abnormal chest roentgenogram. Contrast-enhanced chest computed tomography showed a 62-mm anterior mediastinal tumor. On the basis of the results of 18F-fluorodeoxyglucose positron emission tomography, we suspected a thymic malignant tumor invading the pericardium and left phrenic nerve (Fig. 1). Surgery was indicated.
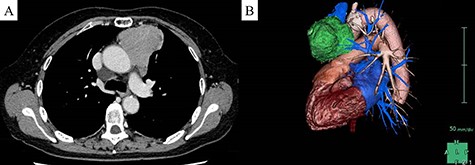
Preoperative image of the tumor. (A) Chest computed tomography revealed a 62-mm anterior mediastinal tumor. (B) Left lateral three-dimensional view of the tumor (green) indicated that the tumor appeared to invade the left phrenic nerve.
The surgery was initiated with a left video-assisted thoracoscopic surgery (VATS) approach in the lateral position (Fig. 2). Because the tumor involved both the left phrenic nerve and pericardium, we sacrificed the phrenic nerve and divided the pericardium to obtain a sufficient surgical margin. The left side of the tumor was dissected.
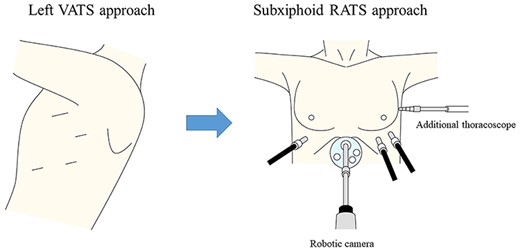
Surgical approach. RATS, robotic-assisted thoracic surgery.
The patient was then placed in the supine position (Fig. 2). A 3-cm skin incision was made below the xiphoid process to perform a subxiphoid approach. Carbon dioxide insufflation was conducted at 8 mmHg. Four ports were inserted to enable the use of the da Vinci Xi robotic system (Fig. 2). We dissected the right side of the thymus.
During robotic surgery, we divided the pericardium to gain an adequate surgical margin. However, the tumor itself was too large to observe the cranial and dorsal sides of the tumor as well as the intrapericardial space. We used conventional thoracoscopy to overcome this limitation. The thoracoscopic image was shown in the TilePro multi-display (Fig. 3). With the aid of both the robotic camera and conventional thoracoscope, the surgeon safely achieved complete resection of the tumor (Fig. 3). The tumor was retrieved via a subxiphoid incision. Finally, we performed pericardial reconstruction under robotic surgery.
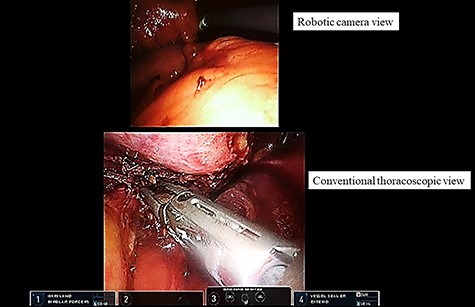
Dual-scopic approach. With the aid of a dual-scopic approach using both a robotic camera and conventional thoracoscopic images, minimally invasive surgical resection of a challenging thymic tumor was achieved.
The patient developed no complications except left phrenic nerve palsy. Pathologic examination revealed a thymic neuroendocrine tumor with no pericardial invasion but with invasion of the left phrenic nerve (pT3N0M0 stage IIIA). The patient received adjuvant radiotherapy and survived for 15 months with no recurrence.
DISCUSSION
We performed minimally invasive surgery for complete resection of a large thymic malignant tumor. Our success was achieved by three important factors: the left lateral VATS approach, the subxiphoid robotic approach, and the dual-scopic approach.
We began with a left unilateral VATS approach because this technique has a great advantage in confirming the ipsilateral phrenic nerve [1]. Confirmation of the left phrenic nerve would have been challenging in the supine position because the tumor would hang down dorsally and limit the surgical view of the phrenic nerve. In addition, the left unilateral approach permitted better observation of the aorta and pulmonary artery. The unilateral VATS approach in the lateral position enabled us to observe the phrenic nerve and the edge of the tumor.
The subxiphoid robotic approach had a crucial role in this surgery. Unlike the unilateral approach, the subxiphoid approach usually offers a better surgical view of the neck and both phrenic nerves [2]. Moreover, the robotic platform makes it easier to conduct complex procedures such as pericardial patch closure.
The dual-scopic robotic approach greatly contributed to the success of this surgery. Even under the robotic subxiphoid approach, the tumor sometimes limited the surgical field of view. In particular, the views of the cranial and dorsal sides of the tumor and the intrapericardial space were limited via the robotic camera because of the large tumor. Additional thoracoscopy provided a good view of the robotic camera’s blind side and thus enabled us to safely perform the robotic procedure. The dual-scopic approach is useful when performing challenging surgery.
Although we applied the left unilateral VATS approach because of the port placement and our familiarity with the procedure, we could have undertaken this surgery solely via the robotic platform. We should reflect on the cost of using both VATS and robotic surgery devices. Despite these drawbacks, we believe that our approach could be an option for challenging mediastinal cases.
In conclusion, we performed dual-scopic robotic thymectomy to achieve complete resection of a malignant thymic tumor. This approach is effective and safe for large thymic tumors.
ACKNOWLEDGMENTS
We thank Angela Morben, DVM, ELS and H. Nikki March, PhD, from Edanz Group (https://jp.edanz.com/ac), for editing a draft of this manuscript.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}