





Abstract
Hemorrhagic cholecystitis is a rare condition with several possible causes. Despite being a difficult diagnosis, it is an important one considering the fatal possibility for the patient. The following is the case of a 68-year-old patient with dual antiplatelet therapy, who underwent coronary angiography and angioplasty in a hypocoagulate setting, developing a hemorrhagic cholecystitis. This article seeks to recognize the importance of this differential diagnosis in hypocoagulated patients with abdominal pain.
INTRODUCTION
Hemorrhagic cholecystitis is a rare condition in which bleeding develops inside the gallbladder with a fatal risk for the patient. In 1948, Sandblom [1] first reported bleeding from the hepatobiliary system to the gastrointestinal tract as hemobilia. In 1979, Shah and Clegg [2] described hemobilia caused by cholecystitis as hemorrhagic cholecystitis.
There are many causes of hemorrhagic cholecystitis. Among them we have the most frequent that is the biliary obstruction by gallstones that counts >50% of the cases [3]. Others less frequent are biliary malignancies, parasitic infections, coagulopathies and trauma [3].
The patient’s symptoms may also vary. Thus, in addition to abdominal pain and hemodynamic instability, patients may also present with hemoperitoneum due to gallbladder perforation or melena or hematemesis due to bleeding to biliary tract or obstruction of biliary tract due to clotted blood [3]. In the diagnosis an abdominal computed tomography (CT) has an important role as we will see later.
Here, we report a case of hemorrhagic cholecystitis in a patient who underwent coronary angiography and angioplasty in a hypocoagulate setting and with dual antiplatelet therapy.
CASE REPORT
A 68-year-old male with arterial hypertension, dyslipidemia, cerebrovascular disease and a history of coronary heart disease, who had already done several percutaneous coronary interventions with stent placement, went to the emergency department with precordial pain and vomiting. At admission, he had an electrocardiogram in sinus rhythm with negative T waves V4–V6, DI and aVL. His blood test revealed leukocytosis 13 790/l with neutrophilia 11 600/l and polymerase chain reaction (PCR) 0.05 mg/dl, with normal cardiac markers. The pain improved with sublingual nitroglycerin. He was admitted and, on the next day, underwent a coronary angiography with angioplasty on the second diagonal of the anterior descending artery with stent placement due to a 70–90% lesion. During the procedure, he performed 5000 Units of heparin and 1 mg of isosorbide dinitrate. After the procedure, he was obnubilated and hypotensive, which improved with fluid challenge. New blood test was taken with evidence of increased leukocytosis to 17.540/l, PCR to 16.4 mg/dl, total bilirubin to 1.52 mg/dl, direct bilirubin 0.74 mg/dl, with normal aminotransferases and gamma-glutamyl transferase. Blood cultures, urine culture, chest X-rays were performed, and empiric antibiotics were started with piperacillin/tazobactam, and the consultation of general surgery was requested. In the evaluation it stands out that the patient was hypocoagulated and with dual antiplatelet therapy, with abdominal pain and defense in the upper quadrants. In blood test he had a slight increase in the international normalized ratio (INR) of 1.26 and in the prothrombin time. An abdominal ultrasound and CT scan (Fig. 1) was performed with evidence of gallbladder hydrops, with high-density contents suspected of thick mud, or hematic content, with a thickened gallbladder wall (~ 4–5 mm), with perivesicular fluid and perivesicular fat densification favoring the hypothesis of acute cholecystitis (Fig. 1). In this context, the patient underwent laparoscopic cholecystectomy on the same day with intraoperative diagnosis of acute gangrenous cholecystitis with intravesicular hematoma and hemoperitoneum (~450 cc) (Fig. 2 and video 1).

Abdominal CT scan showing the gallbladder with high-density contents.
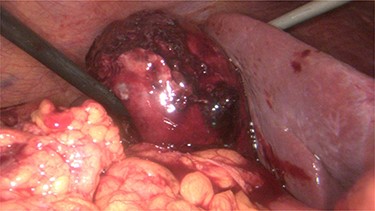
Intraoperative evidence of hemorrhagic cholecystitis.
In the postoperative period, the patient evolved well, ending up being discharged on the ninth day of hospitalization. The gallbladder histology showed intense congestion and extensive hemorrhagic areas compatible with lesions of acute purulent hemorrhagic cholecystitis.
DISCUSSION
Hemorrhagic cholecystitis is a rare cause of gallbladder pathology and of hemobilia. Hemobilia has a described triad of presenting symptoms, including right upper quadrant pain, jaundice and gastrointestinal bleeding [4]. Hemorrhagic cholecystitis is easily overlooked, since its symptoms mimic those of acute cholecystitis with right upper quadrant abdominal pain, liver function impairment, leukocytosis and positive Murphy’s sign [5]. However, patients with hemorrhagic cholecystitis are usually in an unstable life-threatening situation and therefore need urgent care.
As stated earlier, the causes of the development of hemorrhagic cholecystitis may be biliary obstruction by gallstones, biliary malignancies, parasitic infections, coagulopathies and trauma [3]. Pathologically, it is described that it develops due to inflammatory changes that cause ulceration of the mucosa and of the gallbladder vessels, leading to gallbladder rupture and hemoperitoneum [6].
Thus, for the diagnosis, it is important to confirm the presence of bleeding and hematoma in the gallbladder in addition to findings of cholecystitis [7]. For this, patients undergo ultrasound or abdominal CT to aid in the diagnosis. Ultrasound findings can show gallbladder wall thickening, intraluminal membranes and nonshadowing, nonmobile intraluminal echogenic material [8] and how it happened to our patient. In CT scan the findings usually described are dense content with or without layering, which may mimic sludge [9], and if contrast was used, an extravasation of contrast to the lumen may be observed in the arterial phase [10]. Despite these tests, the specific diagnosis of hemorrhagic cholecystitis is sometimes difficult by the similarity with other gallbladder pathologies such as acute cholecystitis [3].
Regarding treatment, endoscopic retrograde cholangiopancreatography (ERCP) plays an important role in cases of hemobilia in stable patients whose cause is not hemorrhagic cholecystitis, because it allows improving the bile flow by removing the calculus or the hematoma impacted in the bile duct [7]. However, in cases of suspected hemorrhagic cholecystitis, urgent cholecystectomy, either laparoscopic or by laparotomy, is the most appropriate treatment. In patients who are not surgical candidates, a cholecystotomy is a valid option [5].
To conclude, this article seeks to recognize the importance of this differential diagnosis in hypocoagulated patients who present with similar symptoms of acute cholecystitis, especially if they are unstable, since the high risk of morbidity advocates a fast surgical decision.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
DECLARATION OF PATIENT CONSENT
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patient understand that his name and initials will not be published, and due efforts will be made to conceal his identity.

{kind=link}
{kind=link}