





Abstract
Surgeons in resource-limited settings have adapted to overcome the challenges of the limitations of resources using different available methods and inventions from the local environment. We report four cases of oesophageal cancer palliatively treated with improvised gastrostomy feeding tubes by using 24Fr urinary catheters, to optimize their nutritional status to withstand chemotherapy/radiotherapy. Two patients managed to begin chemo and radiotherapy, but only one out of the four survived. The aim of this report is to appraise the methods used by surgeons to overcome the challenges they face in clinical practice.
BACKGROUND
Surgical practice in sub-Saharan Africa is faced with many challenges that pose a barrier to meet the desired goals of treatment [1]. Surgical practice in Tanzania as a whole, where the majority of the patients are from rural areas and have limited access to proper health-care facilities and specialist care [2, 3]. A lot of the referral hospitals in resource poor countries lack required equipment due to various socio-economic factors needed to work optimally therefore practitioners modify locally available materials and devices to achieve desired outcomes [1–3]. Here, we mention our experiences of the use of urinary catheters as improvised gastrostomy feeding tubes (GFTs).
CASE PRESENTATIONS
Case 1
A 46-year-old female presented with progressive grade-six dysphagia, vomiting and significant unintentional weight loss. She was wasted and had a BP of 82/53 mmHg, pulse rate of 80 beats per minute, temperature of 36.4°C, saturating at 98% on room air. Her full blood picture was normal with haemoglobin of 12.3 g/dl, Creatinine 41 μmol/l, and urea was <1.0 mmol/l, sodium was 128.2 mmol/l, potassium 3.07 mmol/l. Chest X-ray was normal and the abdominal ultrasound showed no features of intra-abdominal metastasis. Oesophago-gastro-duodenoscopy (OGD) revealed a fungating tumour at 20 cm with almost complete obstruction (Fig. 1) and biopsies taken revealed oesophageal well differentiated invasive squamous cell carcinoma.
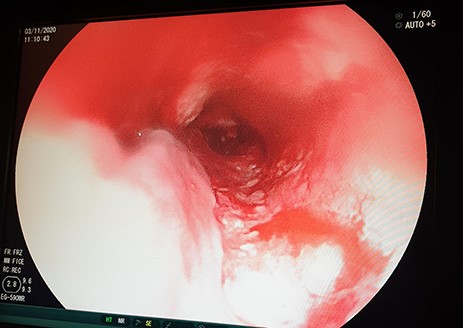
OGD showing a fungating tumour at 20 cm from the upper incisors with almost complete luminal obstruction.
The patient was scheduled for GFT insertion, whereby a 24Fr urinary catheter was inserted via the paramedian incision into the stomach and secured using the Stamm technique (Fig. 2). Intraoperatively the liver had no lesions. The patient was sent to the general ward and semi-solid feeds were initiated through the gastrostomy feeding tube. The patient was discharged on the second day and was instructed to continue with semi-solid feeds, and wound dressing at a nearby health centre. The care-taker was clearly instructed to spigot the catheter after use and to flush the food contents with water after every meal to avoid blockage.
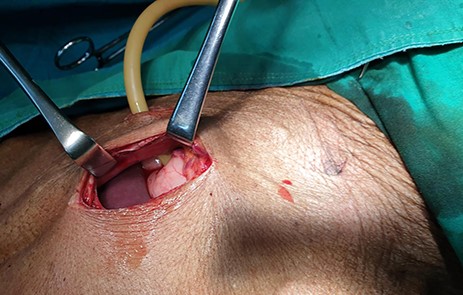
24Fr catheter gastrostomy in Stamm technique.
Two weeks after the GFT insertion, the patient presented to the outpatient clinic with complaints of pus discharge per GFT site. A diagnosis of peristomal surgical site infection was made (Fig. 3), the wound was dressed thoroughly and the patient was sent home with oral antibiotics and had to continue with dressing at a nearby health facility.

Peristomal surgical site infection (arrow).
One-week later, the patient presented to the outpatient clinic with leakage per GFT site. The diameter of the stoma had become wider and a diagnosis of peristomal leakage was made. A purse-string suture was put under local anaesthesia using Nylon 2–0. The patient was then discharged with analgesics and antibiotics.
The patient was referred to the oncology centre for radiotherapy ~4 months after GFT insertion, but she passed away 2 days after the initiation of the first cycle.
Case 2
A 62-year-old male, a smoker and excessive alcohol consumer, non-hypertensive, presented with progressive grade-6 dysphagia that started gradually 7-month ago, associated with unintentional loss of weight. His biological brother was diagnosed with oesophageal cancer 3-year back and had an improvised GFT inserted but passed away shortly thereafter. On general examination he was weak, cachexic, severely pale, not jaundiced, not cyanosed with bilateral pitting lower limb edema with vitals within normal range. Full blood picture initially showed microcytic hypochromic anaemia of 6.4 g/dl, other parameters were essentially normal. Chest X-ray and abdominal ultrasound were essentially normal. Patient did an OGD which revealed at 20 cm a fungating mass partially obstructing lumen (Fig. 4), a biopsy was taken but the scope could not pass through. Histology results for biopsy showed oesophageal invasive squamous cell carcinoma grade 2.
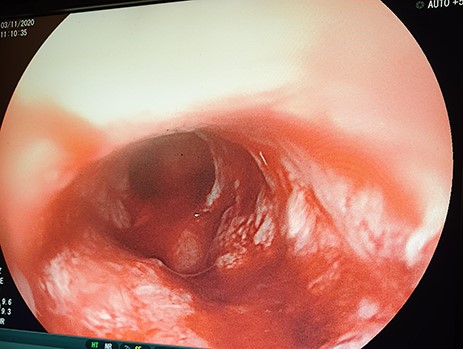
OGD showing a fungating mass partially obstructing esophageal lumen.
Patient was scheduled for GFT insertion, blood transfusion and hematemics were given and control haemoglobin obtained was 13.4 g/dl. Surgery was done and the findings were a collapsed stomach and a non-nodulated liver, a 24Fr urinary catheter was inserted, ballooned and secured using the Stamm technique (Fig. 5). Patient was transferred to the general ward and was discharged on the second day post-surgery.

24Fr catheter as gastrostomy tube.
The patient was reviewed at the outpatient clinic 2-week later and was found to be emaciated, but vitally stable. The patient’s relatives were counselled on the correct nutritional plan and had to be seen in the Oncology unit 3-week later but they were lost to follow up. A phone call was made to the relatives that reported that the patient had passed away 16 days after the final visit.
Case 3
A 62-years-old male who presented with grade-5 dysphagia for 9-month associated with significant unintentional weight loss. He had a positive history of chronic alcohol use and cigarette smoking. No family history of oesophageal cancer. Had an OGD done 2-week prior to admission, which showed a mass obstructing the LES and the scope could not pass through. A biopsy was taken which revealed well differential adenocarcinoma. The lab work up done during admission showed microcytic anaemia of 8.4 g/dl and 400 ml of whole blood was transfused. Other parameters including electrolytes were within normal ranges (Sodium-134.8 mmol/l and potassium-4.66 mmol/l).
He was planned for an improvised GFT insertion. Gastrostomy was done at the body of the stomach and a 24Fr Foley’s urinary catheter was inserted and secured. Around 4 l of amber coloured ascitic fluid was drained. The liver was not nodulated and the mesenteric and paragastric lymph nodes were not palpable. The patient was then discharged after 24-h postoperatively with counselling of wound care and use of semi-solid foods only, through the tube.
The patient was re-admitted 12-day post discharge complaining of leak per GFT insertion site. There was significant peristomal leakage (Fig. 6). He was in a gasping state with cold extremities. The blood pressure and saturation was unrecordable with a respiratory rate of 28 breaths per minute and a weak pulse rate of 50 beats per minute. The chest had basal crepitations on the right lung. Abdominal X-ray showed features of small bowel obstruction with pneumoperitoneum and right sided pleural effusion was noted (Fig. 7). He was supported with high flow oxygen and resuscitated with IV fluids but 3-h post admission the patient succumbed.

Peristomal leakage (arrow).
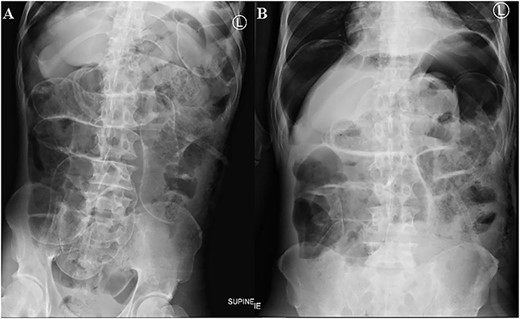
Supine (A) and erect (B) abdomen X-rays show dilated small bowel loops with multiple air fluid levels. Free air seen underneath the hemidiaphragm bilaterally and outlining both sides of the small bowel walls (Rigler sign) suggestive of pneumoperitoneum.
Case 4
A 63-year-old male, 10-day post completion of anti-tuberculosis regimen for pulmonary tuberculosis, known smoker and alcoholic, presented with grade-5 dysphagia associated with food regurgitation, cough and weight loss. On general examination, he was ill looking, cachexic, dehydrated and pale, not jaundiced but no lower limb edema. His vitals were blood pressure of 139/71 mmHg, Temperature of 35.8°C, oxygen saturation of 95% on room air, respiratory rate of 18 cycles per minute and a pulse rate of 73 beats per minute. He had a scaphoid abdomen with tenderness on the right lumbar region. Fine crepitations were heard with reduced air entry on the right side of his chest. Full blood picture was done which was normal with a haemoglobin of 11.3 g/dl, other investigations including renal function tests and liver enzymes were normal. Chest X-ray done showed signs of metastasis (Fig. 8). CT-scan of the abdomen done at the referring hospital with both oral and intravenous contrast reported structures above the diaphragm showing dilated oesophagus measuring 41 × 38 mm due to distal retro-cardiac concentric oesophageal wall thickening amounting to 18 mm with luminal narrowing with possibility oesophageal fistula tract. The gastric cavity was normal without focal lesions. OGD revealed the oesophageal mucosa was hyperemic with a blocking mass at 29 cm from the upper incisors. The scope was able to pass beyond the lesion. The cardiac, fundus and body mucosa was atrophic. There were metaplastic changes at the antrum and pylorus. Multiple biopsies were taken. Histology results revealed oesophageal well differentiated invasive squamous cell carcinoma.

Supine chest X-ray shows patchy infiltrates in the right mid and lower zone with micronodular infiltrates. Micronodules seen in the left lower zones.
The patient was scheduled for GFT insertion. Under aseptic technique, with the patient in supine position, 24 Fr urinary catheter as an improvised GFT was inserted in Stamm manner, haemostasis achieved, abdomen closed in layers and dressed (Fig. 9). There was no ascites and mesenteric lymph nodes were not palpable. After the procedure the patient was discharged home on the second day with analgesics and was booked for a surgical outpatient clinic appointment after 2 weeks.

24Fr urinary catheter as an improvised gastrostomy feeding tube.
The patient was then seen at the clinic after 2 weeks, she was clinically and vitally stable and the GFT was functioning well. The wound had healed, the tube was patent and there was no leakage from the GFT site. Midline sutures were removed and the patient was discharged.
The patient presented to the surgical OPD 3-month later with complaints of GFT blockage at the tip. Under local anaesthesia, the previous tube was removed and another 24 Fr catheter was inserted in a sterile manner and secured and patency was tested. The patient was then discharged and care takers were counselled on use of semi-solid food and to flush the tube with water after every meal.
He was reviewed 3-month later, at the OPD, free from complaints and no leakage with a patent tube. He had already begun his first cycle of radiotherapy.
DISCUSSION
Improvisation is vital to surgical practice in Tanzania and other sub-Saharan countries due to the resource-limited medical facilities hence have led to the optimization of the locally available equipment. This has made the cost of surgery affordable along with satisfaction to the surgeon [1]. Many patients have to bear the costs of the hospital bills and a lot of the time consumables too [1].
Enteral feeding is a common method of nutritional support when oral intake is inadequate. There has been an increase in the use of GFTs due to the introduction of percutaneous methods of tube insertion and use of laparoscopic techniques [4]. GFTs have been used in supportive care, in patients with severe head injury who are on ventilators, as well as in palliative care patients with oesophageal cancer like in our cases [5].
The complications of using a urinary catheter as an improvised GFT were peristomal surgical site infection, peristomal leakage and malfunctioning tube due to blockage. Similar complications have been reported using percutaneous endoscopic gastrostomy tubes, together with colonic perforation, tube dislodgement, buried bumper syndrome and a non-healing stoma [6].
After the improvised GFTs were inserted successfully, the patients were referred back to the oncologists for palliative care using chemotherapy/radiotherapy. Tube feeding enables patients to have a high calorie intake to withstand the complications of chemotherapy/radiotherapy such as loss of fat mass and skeletal muscle mass leading to overt malnutrition [7, 8].
Other types of improvisation reported are underwater seal apparatus for thoracostomy tube whereby water bottles are modified, similar to our cases, large foley catheters are used as gastrostomy tube, the use of urine bags in place of silo for omphalocele closure and usage of nasogastric tubes as ventriculoperitoneal shunts to manage hydrocephalus [1].
CONCLUSION
The scarcity of surgical equipment in Tanzania has given room for improvisation of such items using locally available materials, hence come up with various techniques with local resources in overcoming the limitations imposed by scarcity of certain equipment/devices.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}