





Abstract
Acute bladder injuries are rare and usually occur following significant amount of trauma. It has also been reported to occur in patients with chronic conditions like carcinoma, prolonged indwelling catheters, chronic infections of the bladder among others.
We present a case of an otherwise fit and healthy young woman who presented to our emergency department following an episode of binge drinking and urinary retention. She had a perforation of the bladder following a simple indwelling 18-Fr Foley’s catheter insertion.
In our knowledge, this is probably the first case to be described for such an injury with such mechanism.
INTRODUCTION
Bladder injury/perforation occurs very rarely, and most common cause is blunt abdominal trauma.
Iatrogenic bladder perforation due to Foley’s catheter insertion is an extremely rare phenomenon. There is a paucity of literature regarding any specific cause. Almost all the cases reported so far had some known pre-existing medical conditions that were hypothesized to be the cause of perforation. We describe a case of bladder perforation in a fit, healthy young female following insertion of Foley’s catheter.
CASE
A 29-year-old Caucasian female presented to our hospital with suprapubic pain and urinary retention following binge drinking of around 10 standard drinks of alcohol the night before. The patient presented following three episodes of vomiting at home. The patient denied any fevers, per-vaginal discharge, dysuria, frequency or haematuria. The patient did not have any other significant past medical history and was not on any regular medications. Only previous surgical history consisted of an open appendicectomy as a teenager.
The patient suggested to have a stable partner and denied any current/previous sexually transmitted infections.
On presentation, routine pathological tests suggested normal full blood count and renal function with a leukocyte count of 4.22 × 109, haemoglobin of 124 g/l and a serum creatinine of 52 μmol/l. Liver function tests were neither indicated nor performed.
A bedside bladder scan suggested a distended urinary bladder with >1 l of fluid in it. To relieve her symptoms, a Foley’s catheter (18 Fr) was inserted. The patient, however, failed a trial of void and another Foley’s catheter (18 Fr) was inserted. The patient was kept under observation for the next 24 hours as her pain continued, and haematuria was witnessed in her indwelling catheter (IDC).
The patient proceeded to have a computed tomography (CT) of her abdomen, which could not suggest any reason for her symptoms. However, she did not improve clinically, and thus, we organized an ultrasound of the abdomen and pelvis to rule out any biliary pathology that could have been missed with CT scan (Fig. 1).

Abdominal CT showing urinary catheter protruding through dome of bladder.
The ultrasound scan was unequivocal, only suggesting some free fluid in the abdomen and pelvis, which was not present in the CT.
The patient then underwent a laparoscopy, which confirmed a bladder dome perforation with the tip of the Foley’s catheter. Her pelvic organs appeared normal. Incidentally, violin-like liver adhesions were found during her laparoscopy in keeping with Fitz-Hugh–Curtis syndrome (FHCS). The bladder dome was repaired laparoscopically, and peritoneal fluid was sent for microscopy and culture. Retrospective re-evaluation of CT images confirmed the diagnosis (Figs 2 and 3).
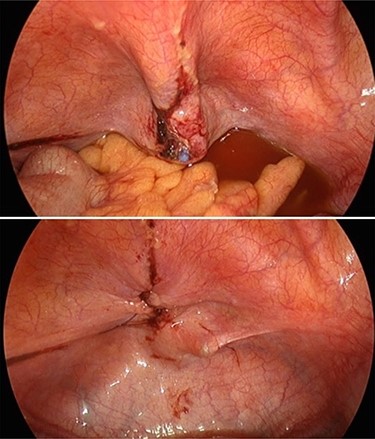
Intraoperative photo showing tip of Foley catheter protruding through bladder wall and subsequent repair.

Intraoperative photo showing violin-like adhesions on liver.
The patient recovered well post-operatively and was discharged home 1 week later with negative peritoneal fluid cultures.
DISCUSSION
Bladder Injuries are a rare problem often caused by high-impact blunt trauma. Other causes include—carcinoma, chronic catheterization, intermittent self-catheterization and more [1]. Diagnosis can be confirmed using X ray or CT with or without cystography or otherwise through intra-abdominal evaluation [2].
Iatrogenic injuries are mostly associated with increased age, previous radiotherapy/chemotherapy and smoking [3]. It is most commonly associated with abdominal and pelvic operations with an incidence of ~1 in 1000 [3]. Catheterization is a very rare cause of bladder injury with only a handful of reported cases.
Furthermore spontaneous bladder rupture is an extremely rare problem that can also cause bladder injury [4]. Interestingly, there have been around 10 reported cases of binge alcohol consumption inducing spontaneous bladder rupture in the literature, with one hypothesizing overdistension of the bladder and thinning of the bladder wall inducing the injury. Our patient’s bladder did not rupture spontaneously, with the IDC protruding into the peritoneal cavity; however, her binge alcohol consumption may have distended and thinned her bladder wall, predisposing the injury.
An incidental operative finding was the presence of violin-like adhesions found between her liver and anterior abdominal wall suggesting FHCS. FHCS is a common manifestation of previous pelvic inflammatory disease (PID) associated with inflammation of the liver capsule and violin-like adhesions [5]. It is prevalent in ~10–15% of women with PID and is suggested to have a variety of clinical presentations ranging from acute right upper quadrant pain, fevers and vomiting, to no symptoms at all [6]. We are unsure whether this could have also contributed to the thinning of her bladder wall predisposing it to a higher chance of perforation even from such a mild intervention such as Foley’s catheter placement.
Bladder injuries irrespective of their cause should be managed promptly by surgical intervention to avoid progressive leakage of urine into the abdomen leading to increased morbidity [7].
Urinary retention following binge drinking is a common presentation and placement of Foley’s catheter is a commonly performed procedure. However, a high index of suspicion is needed in case of patients presenting with similar symptoms, which are not resolved, or they worsen with catheter placement so as to not miss this diagnosis.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}