





Abstract
Chylous ascites (CA) results in a thick white ascitic fluid, akin to milk. It is most commonly caused by malignancy and cirrhosis in adults. Here we present only the second reported case of primary small bowel volvulus resulting in CA in the virgin abdomen. The patient presented with acute onset, severe abdominal pain. She underwent an urgent laparotomy where a large volume of CA was drained. The bowel and its mesentery were congested with chyle and stained white. Following detorsion the bowel returned to normal, and the patient recovered well. Here we review the radiological findings and aetiology of CA, due to small bowel volvulus. This case highlights the importance of timely surgical intervention in patients with volvulus to prevent irreversible bowel ischaemia and if untreated, perforation.
INTRODUCTION
Chyloperitoneum or chylous ascites (CA) is caused by the leakage of lipid-rich chyle into the peritoneal cavity, resulting in yellow-white peritoneal fluid [1]. It is responsible for 0.001–0.005% of hospital admissions [2, 3]. There are many aetiologies by which CA may arise. Trauma, malignancy, cirrhosis, fibrosis, iatrogenic injury, radiation, congenital defects as well as a number of idiopathic cases have been recognized [2–10].
Three pathogenic mechanisms have been described for CA. Lymphoperitoneal fistula in which chyle leaks from the retroperitoneal lymphatics via an abnormal tract [2, 3]. Exudation of chyle through large retroperitoneal lymphatics without fistula and blockage of the lymphatics at the base of the mesentery, cisterna chyli causing leakage of chyle from dilated lymph channels within the bowel and its mesentery [2, 3]. Malignancy and cirrhosis are responsible for the majority of cases in adults, whereas in children congenital abnormalities account for the majority [1–3]. Mortality rates as high as 50–70% have been reported in adults and its treatment is aetiology dependent [1–3].
CASE REPORT
A 79-year-old woman presented to the emergency department with 2 hours of sudden-onset, severe epigastric pain. The pain was constant and severe. She reported feeling bloated but had been passing hard bowel motions in the days prior and had passed flatus that morning. There was no history of weight loss or rectal bleeding. Past medical history included coronary artery disease, hypertension, hypercholesterolaemia and blastocystis. She had no history of abdominal surgery and was an independent, non-smoker.
On examination she was mildly tachypnoeic, with normal oxygen saturations, heart rate was 74/min, with a blood pressure of 151/80 mmHg. On palpation, she was grossly distended, guarding and peritonitic throughout with no palpable hernias. Blood tests revealed an elevated white cell count of 13.4 × 109/l and a lactate of 2.3 mmol/l. An urgent computerized tomography (CT) scan of the abdomen and pelvis was performed. The CT demonstrated a large volume of free intraperitoneal fluid, with multiple loops of distended small bowel (Figs 1 and 2) without pneumoperitoneum. Although not noted in the report, there was concern about a ‘swirl’ in the mesentery, raising the possibility of a small bowel volvulus (SBV).
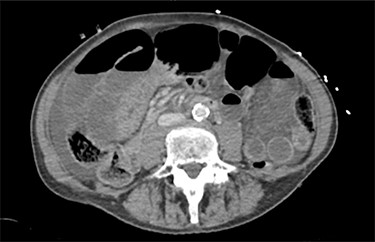
The patients CT scan, axial slice showing distended loops of small bowel and free fluid.

The patients CT scan, coronal slice.
The patient was taken urgently to theatre for an exploratory laparotomy. Upon entering the peritoneal cavity, a large volume of white liquid was drained. Biochemical analysis of this fluid confirmed triglycerides of 770 mg/dl. Cytology was negative for malignant cells and no organisms cultured. The small bowel was distended, its mesentery congested and white (Fig. 3), with a volvulus at the root of the small bowel mesentery. The volvulus was detorted, congenital adhesions near the base of the mesentery divided after which the mesentery and bowel returned to normal colour. The small bowel walked from terminal ileum to duodenal–jejunal flexure with no further obstruction point evident. Inspection of the rest of the abdomen was unremarkable. The abdomen was washed, and the fascia was closed with 0-nylon and the skin closed with staples. On Day 4 a repeat CT scan demonstrated an ileus. Her ileus settled with conservative management and on Day 7 after surgery was discharged tolerating a full diet. Four weeks later she was reviewed in the clinic and was recovering well.

Photo taken at laparotomy demonstrating small bowel and mesentery congested with chyle.
DISCUSSION
Analysis of the fluid drained from peritoneal cavity confirmed the diagnosis of true CA. Peritoneal fluid with a triglyceride content >110 mg/dl is considered true CA [1]. Two other causes of this yellow-white fluid are described. Pseudochylous ascites occurs when peritoneal fluid is coloured by pus, whereas chyliform ascites describes the lecithin-rich fluid from the degeneration of cells due to malignancy or peritonitis [3].
In the case of our patient primary SBV was the causative pathology. Primary SBV occurs in the absence of a structural cause in a normal abdomen [10–12]. Secondary SBV describes volvulus occurring as a sequelae of previous surgery or alternate pathology [10–12]. Primary SBV has been associated with the intake of large volumes of fibre, following a period of fasting [10]. Subsequently, primary SBV is more prevalent in societies that practice intermittent fasting [11]. It is thought the large bolus of food acts as a lever in the jejunum, by dropping into the left lower quadrant, forcing the empty bowel loops to rotate around the base of the mesentery [13]. A long, narrow-based small bowel mesentery has also been thought to predispose to SBV [10–13]. In our case, neither factor was noted, nor was single causative factor identified. The patient was known to have the bowel parasite blastocystis; however, this has been not been reported to cause SBV.
The volvulus resulted in compression of the lymphatics in the base of the mesentery. The mesentery became engorged with chyle, resulting in the white staining seen. When torsion of the mesentery occurs, there is disruption to the venous drainage of the bowel. Ischaemia and later necrosis occur, which, if left untreated, results in perforation with subsequent poor outcomes [12, 14].
Prompt recognition and treatment of SBV is paramount. In our case the initial examination, biochemical and radiological findings were concerning for ischaemic bowel, hence the urgency with which the patient was taken to theatre. In primary SBV, urgent laparoscopy or laparotomy, detorsion and careful inspection of the bowel is the treatment of choice [14]. Congenital adhesions should be divided if contributing to the volvulus [12]. Any non-viable segments should be resected and anastomosed as the patient’s condition permits. In patients with secondary SBV the surgery should also address the causative pathology. In our case, following detorsion of the volvulus, the bowel and its mesentery returned to normal colour. Timely surgical intervention avoided the need for resection and the morbidity associated with it. Reported mortality rates for SBV vary between 9–35%; this rises further in the presence of non-viable bowel necessitating resection [10–12].
This case represents only the second reported case of primary SBV causing CA in the virgin abdomen. Timely recognition and intervention in SBV are paramount to a successful outcome. The chylous fluid and congested white bowel and mesentery seen at operation in CA secondary to SBV bears remembering.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}