





Abstract
Rib tumors are rare. They can present with wide varieties of symptoms and differentiating benign from malignant lesions is challenging. A careful history and supporting investigations can help to reach the definite diagnosis. Surgical resection is the treatment of choice with excellent prognosis. A total of four patients were operated for the management of rib tumors over a period of 5 years at our institution. All four were benign lesions and included simple bone cyst, fibrous dysplasia with aneurysmal bone cyst, aneurysmal bone cyst and enchondroma. There were three male and one female. None of them is having recurrence till now. Surgical resection is the treatment of choice for benign rib tumors as it provides diagnostic and curative treatment.
INTRODUCTION
Primary chest wall tumors are infrequent, accounting for only 0.04% of all new cancers diagnosed and 5% of all thoracic neoplasms [1–3]. Primary tumors of the rib encompass 5–7% of all primary bone neoplasms but contribute 50% of bony malignant tumors and the majority of benign bony tumors of the chest wall [2, 4]. Most of the rib lesions are secondary malignant tumors, metastatic involvement or direct invasions from adjacent malignancies such as breast cancer, lung cancer, mesothelioma and mediastinal tumor. Tumors arising from the rib are as likely to be benign as malignant when metastases are excluded [2]. Fibrous dysplasia and enchondroma are the most frequently detected benign rib lesions [4].
Typically, patients with rib lesions present with a palpable mass, pain or both. Asymptomatic patients are diagnosed incidentally after routine imaging as part of a screening or investigation of an unrelated condition in lesser occasions [1, 2].
Rib abnormalities are often primarily identified on chest radiography. However, computed tomography (CT) and magnetic resonance imaging are valuable in determining the boundary of tumor and detecting invasion to the adjacent organs, nerves and vessels [4]. Management consists of wide resection in cases of malignant rib lesions with possible reconstruction of the thoracic wall, and resection of only the affected rib in cases of benign rib lesions [5].
Rib tumors can present both a diagnostic and therapeutic dilemma because of their rarity and often benign presentation. Here, we present four cases of benign rib tumors managed over a period of 5 years at Tertiary Care Centre of Nepal, with a purpose to review their clinical, radiological and pathological features, as well as the early and long-term results of surgical management.
CASE SERIES
Case 1
A 15-year-old girl present with lump in right chest with gradually progressing discomfort of 6-month duration. The discomfort was constant with intermittent exacerbation. She had no history of trauma or prior chest surgery, and her past medical history was unremarkable. Her physical examination revealed a palpable mildly tender mass on sixth rib on anterolateral wall of the right chest. Her routine laboratory test results, including complete blood count, erythrocyte sedimentation rate, renal function test and liver function tests, were all within normal range. Chest radiograph performed showed destruction of right sixth rib (Fig. 1A). CT chest revealed 36 × 30 × 80 mm well-defined large uniloculated cystic lesion of the sixth rib involving anterolateral part and abutting the costochondral junction (Figs 1B and C). She underwent surgery after all diagnostic investigation was completed.
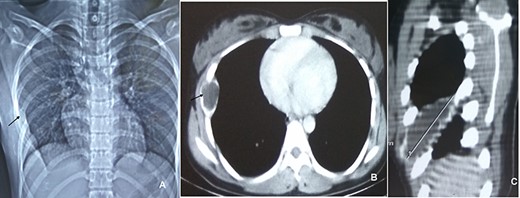
CXR (A, arrow) showing mass lesion in sixth rib. CT chest axial (B, arrow) and saggital (C) showing uniloculated bone cyst.
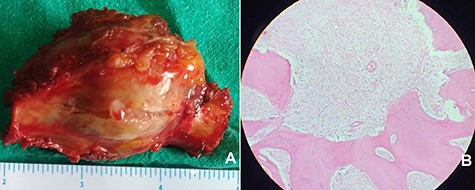
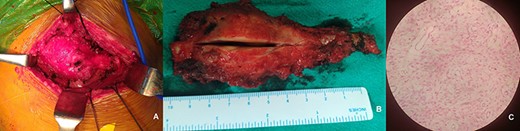
A right anterolateral thoracotomy was done and the right sixth rib with cyst segment was exposed. It was extending from near to costochondral junction to posterior third of the rib. The underlying visceral pleura and lung was free. The entire cyst was resected along with the adjacent parietal pleura and normal rib segment. The chest was closed primarily without any reconstruction. The cut section of specimen revealed cystic space covered with thin bony shell and filled with serous fluid (Fig. 2A). Histopathology confirmed the simple bone cyst (Fig. 2B). Her post-operative course was uneventful and discharged on 4th post-operative day without any complaints. After 4 years of follow-up, she is doing well without any recurrence.

(A) resected specimen of simple bone cyst. (B) Photomicrograph (200×) of rib revealing uniloculated cyst lined by flattened epithelium.
Case 2
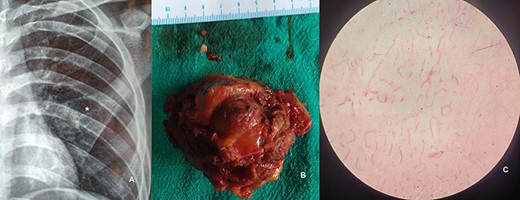
A 43-year-male presented with complain of incidentally detected swelling on the right lateral chest wall of 6-month duration not associated with pain or tenderness. He denied any history of trauma or prior chest surgery, and his past medical history was unremarkable. It was slowly increasing in size. A physical examination revealed a palpable non-tender mass of fifth rib on anterolateral wall of the right chest. His all routine laboratory test results were within normal range. Chest radiograph performed showed lytic lesion of right fifth rib (Fig. 3A). CT chest revealed 40 × 36 × 60 mm well-defined large hypodense cystic lesion of the fifth rib involving anterolateral part (Fig. 3B). Fine needle aspiration cytology was inconclusive. A right anterolateral thoracotomy was done and the right fifth rib was excised. The mass was resected totally along with the adjacent parietal pleura and normal rib segment (Fig. 4A). The chest was closed primarily and did not require any reconstruction. The cut section of specimen revealed gelatinous material covered with thin bony shell. Histopathology confirmed the mass to be enchondroma (Fig. 4B). His post-operative course was uneventful and discharged on 3rd post-operative day without any complaints. After 3 years of follow-up, he is doing well without any recurrence.
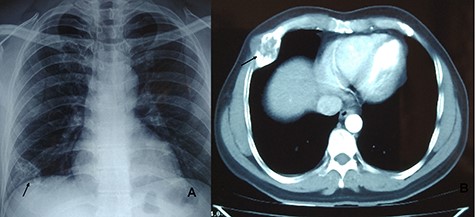
CXR showing lytic lesion of right fifth rib (A). CT chest showing well-defined large hypodense cystic lesion of the fifth rib involving anterolateral part (B).
Resected specimen of enchondroma (A). H&E stained 40× photomicrograph suggestive of enchondroma (B).
Case 3
A 29-year-male presented with complain of swelling on the right posterolateral chest wall of 3-month duration associated with mild pain on and off. There was no history of trauma, and his past medical history was non-contributory. It was slowly increasing in size. His physical examination revealed a mildly tender palpable mass of tenth rib on posterolateral wall of the right chest (Fig. 5A). His all routine laboratory test results were within normal range. Chest radiograph performed showed vague lesion of right tenth rib. CT chest revealed 11 × 4 cm lytic lesion of the tenth rib involving posterolateral part (Figs 5B and C). Fine needle aspiration cytology was hemorrhagic. A right anterolateral thoracotomy was done and the mass present in posterolateral part of right 10th rib was excised (Fig. 6A). The underlying visceral pleura, lung and diaphragm were free. The mass was resected along with the adjacent parietal pleura and normal rib segment (Fig. 6B). The cut section of specimen revealed hemorrhagic material covered with thin bony shell. Histopathology confirmed the mass to be Fibrous dysplasia with aneurysmal bone cyst-like areas (Fig. 6C). His post-operative course was uneventful and discharged on 3rd post-operative day without any complaints. After 2 year of follow-up, he is doing well without any recurrence.
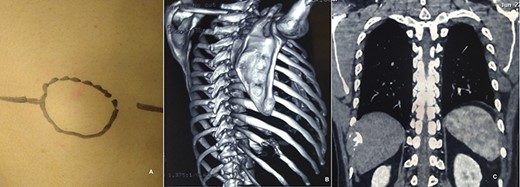
Mass in right posterolateral wall (A). CT chest showing lytic lesion of right tenth rib (B and C).
Intra-operative image showing mass in right tenth rib (A). Resected specimen (B). H& E stained 40× photomicrograph of specimen suggestive of fibrous dysplasia (C).
Case 4
A 35-year-male presented with complain of swelling on the left anterolateral chest wall detected incidentally on routine chest X-ray. It was associated with mild pain on and off. He denied history of trauma or chest surgery, and past medical history was non-significant. It was slowly increasing in size. A physical examination revealed a palpable mass of third rib on lateral wall of the right chest. His biochemistry and hematological laboratory test results were within normal range. Chest radiograph performed showed destruction of the left third rib (Fig. 7A). CT chest revealed 10 × 6 cm lytic lesion of the third rib involving anterolateral part. His fine needle aspiration cytology was negative for malignancy. The left third rib was excised via left anterolateral thoracotomy. The underlying visceral pleura and lung was free. The mass was resected along with the adjacent parietal pleura and normal rib segment (Fig. 7B). The cut section of specimen revealed hemorrhagic material covered with thin bony shell. Histopathology confirmed the mass to be aneurysmal bone cyst (Fig. 7C). His post-operative course was uneventful and discharged on 3rd post-operative day without any complaints. After 1 year of follow-up, he is doing well without any recurrence.
CXR showing mass lesion of left third rib (A, asterisk). Intra-operatice specimen of resected third rib (B). H&E stained 40× photomicrograph of specimen suggestive of aneurismal bone cyst.
DISCUSSION
Rib tumors are uncommon, with an incidence of less than 1% in the general population [1, 2]. Malignancy among them is ominously more common than benign lesions. However, among the patients evaluated in their study by Sakellaridis et al., those with benign tumors were more common [6]. In line with aforementioned study, all of our reported cases were benign cases.
It is reported that rib tumors occur with equal gender distribution [5]. In our series, there was male predominance. Fibrous dysplasia and enchondroma are the most common benign lesions, with aneurysmal bone cyst and simple bone cyst considered as rare benign rib tumors [1, 2, 4]. Our case series reported all of these varieties of benign rib tumors.
Benign rib tumors can present in various ways. Asymptomatic patients diagnosed incidentally after routine examination as part of a screening or investigation of an unrelated condition are generally limited [1, 2]. However, two out of four cases in our study were detected incidentally. Mostly, patients present with palpable enlarging mass. Pain is the second most common symptom with which the patients present. Pain is often vague and diffuse, which affects a particular region of the chest, which is often accredited to a musculoskeletal cause, such as arthritis or recent trauma [1]. Consistent to former findings, our patients presented with a mass and pain or discomfort as their chief complaints. However, no any history of trauma was associated with either of the cases.
The diagnosis of a rib tumor necessitates a careful history and physical examination followed by a plain chest radiographs and a CT scan. A history of trauma to that specific area may imply that the lesion is benign and probably a posttraumatic fibro-osseous lesion. Physical examination may or may not reveal a mass or tenderness and the examination should incorporate inspection for enlarged lymph nodes. The diagnosis of the reported cases in our study was assisted by plain chest radiographs and CT scan and confirmed with histopathology after resection.
Plain chest radiographs (CXR) are the first radiological studies used in the diagnosis of rib tumors. Moreover, some tumors are incidentally found on CXR. Although insufficient as the sole imaging modality in the current era of advanced imaging techniques, CXR can still provide useful evidence about the tumor: the size, location, calcification, ossification, bony involvement, presence of enlarged mediastinal lymph nodes and, if any, of large pulmonary metastases can all be ascertained [2, 7, 8].
The need of pre-operative biopsy remains debatable. Fine-needle aspiration or non-excisional biopsy of the rib tumor should be performed carefully. Some authors consider that fine-needle biopsy must be discouraged since diagnosis by cytologic specimen is sometimes sub-standard. Out of the four cases, three of them were considered for fine-needle aspiration cytology, and none of them showed features of malignancy. Incorrect diagnosis due to inadequate tissue specimen may even lead to less than optimal treatment and worse prognosis. The risk of implantation of tumor tissue along the needle track after aspiration biopsy is remarkable and makes it an unpopular preoperative diagnostic tool [1].
Rib tumors should be contemplated malignant until proven otherwise, due to difficulty in differentiating benign from malignant tumor preoperatively. For benign or metastatic rib tumors, surgery must comprise of wide resection of the involved ribs with 2–3 cm free margins to be considered as adequate. All of the cases in this report were surgically resected with ample of free margins.
The overall 5-year survival after resection of primary chest wall neoplasm is roughly 60%. Recurrence can occur in up to 50% of patients, with a subsequent 5-year survival of 17%. The prognosis of benign tumors after surgical excision is consistently excellent [1, 9, 10]. All reported cases are followed up and are free of symptoms, thereby, emphasizing the good prognosis after surgical resection in benign rib tumors.
In conclusion, benign rib tumors are rare. Proper history and clinical examination can be elicited to diagnose such lesions along with radiological investigations. Surgery consists of wide resection of the tumor with free margins, in order to provide the best chance for cure and to ensure a good prognosis in long term.
The authors received no financial support for the research, authorship and/or publication of this article.
Both the authors declared no potential conflict of interests with respect to the research, authorship and/or publication of this article.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}