





Abstract
Bilateral femoral hernia is a peculiar clinical condition, with female predominance, with only a few cases reported in the literature. There are only two cases of bilateral strangulated femoral hernias, and these occur solely in females. To our knowledge, in the present manuscript, a bilateral strangulated femoral hernia in a male patient is reported for the first time. A 68-year-old male proceeded to the emergency department of our institution with symptoms of bowel obstruction. Abdominal computed tomography, magnetic resonance imaging and subsequent emergency laparotomy revealed obstruction of the sigmoid colon and simultaneous necrosis of several loops of the small intestine due to bilateral strangulated femoral hernia. The operation was uneventful. Despite the scarcity of this clinical condition, surgeons’ awareness is fundamental, in addition to deep knowledge of the pathology and the anatomy of femoral hernias, in order to diagnose and treat adequately strangulated and incarcerated femoral hernias.
INTRODUCTION
Bilateral femoral hernia is an extremely rare clinical condition, with only a few cases reported in the literature [1], especially for male patients [2, 3]. Femoral hernias are prone to strangulation because of the rigid femoral ring and the narrow femoral canal [3]. However, there are only two cases of bilateral strangulated femoral hernias, and these occur solely in females [4, 5]. To our knowledge, in the present manuscript, a bilateral strangulated femoral hernia in a male patient is reported for the first time in the literature. The current study provides evidence of this peculiar clinical occurrence and highlights its prompt diagnosis and surgical management.
CASE REPORT
A 68-year-old male proceeded to the emergency department of our institution with perpetual and penetrating abdominal pain, abdominal distention, vomiting and constipation for 2 days. His medical history was unremarkable without previous surgeries, hospitalizations or any co-morbidities. His body mass index was 19.7 kg/m2. Physical examination certified abdominal tenderness, peritonism and the presence of two lumps in the anatomic region of the right and the left femoral triangles. In addition, bruit was audible over the left lump.
Laboratory examination revealed increased levels of C-reactive protein, LDH and neutrophils. Subsequent computed tomography (CT) and magnetic resonance imaging (MRI) of the abdomen and the pelvis indicated bowel obstruction of the sigmoid colon and obstruction of several loops of the small intestine as well (Fig 1). Herein, the patient underwent emergency laparotomy 2 h after he was initially assessed by the surgical team.
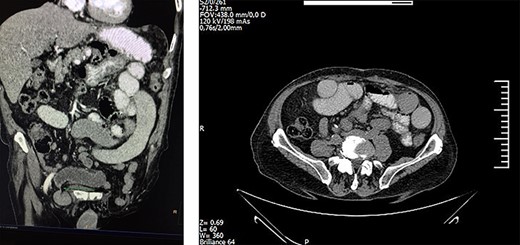
Abdominal CT indicating bilateral bowel obstruction.
Surgeons performed high McEvedy’s approach and identified a small knuckle of gangrenous bowel strangulated in the right femoral hernia, while the left one included a small part of the sigmoid colon, which was still viable (Fig 2). The ischemic bowel loops were dissected off, and an anastomosis was immediately performed via a stapler device.
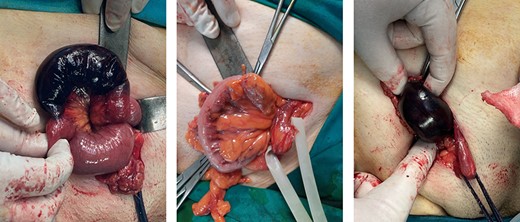
Strangulated bilateral femoral hernia; the right hernia included gangrenous loops of the ileum and the left one included a small part of the sigmoid colon.
Finally, both femoral regions where meticulously examined and femoral canals were repaired with prolene interrupted sutures. The operation was uneventful, and the patient was admitted to the ICU for almost 6 h until it was asserted that he was hemodynamically stable. The patient was discharged with instructions the sixth post-operative day. At a 6-month follow-up, the patient presented full recovery without any complications.
DISCUSSION
The presence of the bilateral femoral hernia is extremely rare since only a few cases are documented in the literature [1, 2, 4], with minor reports of male patients [3, 4]. Furthermore, bilateral strangulation is documented only for a female patient [3, 5]. To our knowledge, the present case is the first reported case of a male patient presenting with simultaneously strangulated bilateral femoral hernia with strangulation of the sigmoid colon and the ileum.
Femoral hernias, and especially the bilateral ones, are present with a female predominance [1], and their presence in males is typically related to previously operated inguinal hernia [6]. In the presented case, though, the patient had no medical history of inguinal hernia and neither clinical conditions causing increased intra-abdominal pressure.
According to the literature, although the etiology of femoral hernias remains vague, the weakness of the transversalis fascia is estimated as a potential etiological factor [7].
Femoral hernias may present reducible, irreducible, incarcerated or strangulated, as in the presented case [1]. When remaining asymptomatic, their differential diagnosis may be challenging since mimicking venus aneurysms of the sapheno-femoral anastomosis, especially for obese patients [1, 3]. Ultrasonography, CT and MRI are extremely helpful for the adequate differential diagnosis [4].
Last but not least, femoral hernias are extremely prone to strangulation due to the narrow femoral canal and femoral ring, and the area of obstruction is typically the femoral ring or a region, 1.5 cm below [3, 8]. When strangulated, femoral hernias should be considered as surgical emergencies since the mortality remains high [1, 9].
There are several documented surgical approaches for the repair of a femoral hernia depending on the type of the hernia and the surgeon’s experience [1, 4]. Nevertheless, if feasible, laparoscopy is more favorable due to alleviating the probability of recurrence and the post-operative pain [4]. On the other hand, high McEvedy’s laparotomy as performed in the presented case, permits adequate access into the peritoneal cavity, overview of the bowels and meticulous, safe and handful resection, when essential [4].
Repair of the femoral defect may be performed with mesh or primary sutures, as in the presented case [4]. However, mesh is suggested to be avoided in cases of emergency because of the potentiality of post-operative abscess or even peritonitis.
Conclusively, it is suggested that we describe for the first time a case of bilateral strangulated femoral hernia in a male patient, with strangulation of both the ileum and the sigmoid colon. Despite the scarcity of this clinical condition, surgeons’ awareness is fundamental, in addition to deep knowledge of the pathology and the anatomy of femoral hernias, in order to diagnose and treat adequately strangulated and incarcerated femoral hernias.

{kind=link}
{kind=link}