





Abstract
Retrocaval ureter or circumcaval ureter is considered a rare congenital anomaly. We reported a case of 48-year-old woman who presented with right flank pain. In investigations, we found a retreocaval ureter that was treated surgically. In conclusion, retrocaval ureter is rare cause of flank pain and one of the challenging cases for urologists that needs careful investigations.
INTRODUCTION
The retrocaval ureter is a rare congenital entity resulting from an abnormal development of the inferior vena cava (IVC) [1].
In this condition, the proximal ureter passes posterior to the IVC at the level of the third lumbar vertebra to lie at its medial aspect, whereas the distal part returns to its normal position crossing the IVC from medial to lateral aspect anterior to the lower part of the IVC. Obstruction is usually at the retrocaval segment of the ureter as it lies compressed between the IVC and the body of the third lumbar vertebra [2].
Although it is a congenital anomaly, but patients usually present in third and fourth decades of life with intermittent flank or abdominal pain or dull ache due to ureteric obstruction and associated hydronephrosis [3].
We present here a case of 48-year-old woman with retrocaval ureter, which was the first case to be treated successfully at Aleppo University Hospital.
CASE PRESENTATION
A 48-year-old woman came to our outpatient clinic, Department of Urology at our hospital with intermittent right flank pain for three months. Her past medical history was unimportant, except that she had allergic bronchitis. Her past urological history was remarkable for recurrent urinary tract infection treated successfully with short course of antibiotics. There was no hematuria or other lower urinary tract symptoms. General physical examination showed mild tenderness in the right flank. Other systems were normal. The results of the laboratory tests are shown in Table 1.
The results of the laboratory tests
| Hemoglobin | 9.9 |
| Wight blood cells (WBC) | 10.200 |
| Platelets | 350.000 |
| Glucose | 103 |
| Creatinine | 0.9 |
| Urea | 38 |
| Urinalysis | |
| Red blood cells | 2–3/HPF |
| WBC | 10–12/HPF |
| Calcium oxalate | + |
HPF, high power field.
An abdominal ultrasonography revealed moderate right renal hydronephrosis and proximal hydroureter. A routine X-ray kidney-ureter-bladder (KUB) was normal. Intravenous urography (IVU) showed right renal hydronephrosis with delayed excretion and drainage (grade II) with s shape of the upper segment of the right ureter (Fig. 1). Then, the patient underwent right retrograde ureteroscopy with contrast to confirm the findings. Depending on these results, we decided to do the surgery for a right retrocaval ureter. After taking the patient consent, we had used Kocher approach to reach retroperitoneal space. After isolating of the right renal pelvis and ureter, the segment of retrocaval ureter was lower the ureteropelvic junction ~3 cm and dilated. We transected the pathological segment (~3 cm) of the ureter and then we did ureteropelvic end-to-end anastomosis. We inserted a double-j stent (Fig. 2). After a month, there was no hydronephrosis, and we removed the double-j stent. Six months follow-up demonstrates complete resolution of this pathology.
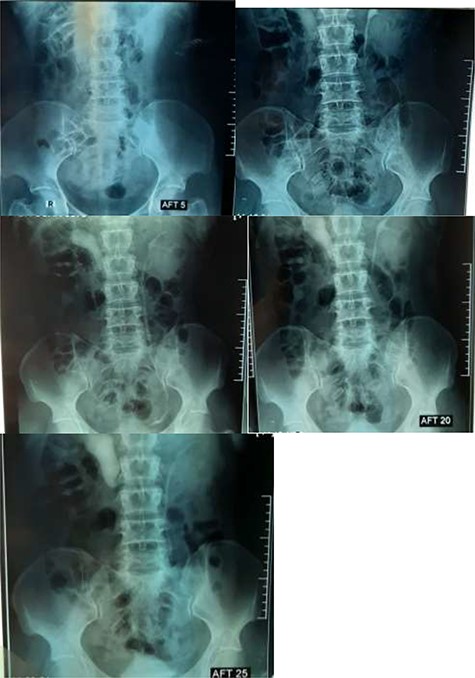
IVU shows S-shaped sign.

KUB demonstrates right double-j stent.
DISCUSSION
Retrocaval ureter is a rare congenital anomaly that is caused by an abnormal formation of infrarenal IVC from anteriorly located subcardinal vein instead of supracardinal vein, which are located posteriorly. It entraps a segment of the proximal ureter, resulting in the ureter wrapping around the IVC. Therefore, it is also known as circumcaval ureter or preureteral vena cava. This anomaly is rare with an incidence of 0.06–0.17% worldwide. It is three times more common in males than in females [4].
In the literature, retrocaval ureter has been classified into two clinical types, in accordance with the common radiological appearance. The more common type 1 (also named ‘low loop’) is characterized by the so-called ‘typical S’ or ‘fishhook’ deformity of the ureter to the level of the obstruction [3]. In this case, the abnormality was type 1 and the obstruction was at the right side beside the lateral margin of the IVC at the level of lumbar vertebrae L2–L3.
Patients generally present symptoms in the third or fourth decade of life, especially symptoms related to ureteral obstruction and hydronephrosis, such as right flank pain, repetitive urinary infections and nephrolithiasis; patients may complain of hematuria [1]. The patient in this case presented with interrupted flank pain, and no hematuria had been recorded.
The imaging studies are important for an accurate preoperative diagnosis and successful surgical management. Abdominal ultrasound demonstrates hydronephrosis and proximal hydroureter without calculus. The IVU shows typical ‘fish hook’ or ‘J’- or ‘S’-shaped deformity in the proximal dilated ureter with moderate hydronephrosis. Nowadays, computed tomography urography is preferred over IVU or retrograde pyelography (RPG) as it may depict the anomaly in three dimensions giving the most ‘wholesome’ solution to its diagnosis [3]. For our patient, ultrasonography revealed moderate right renal hydronephrosis, and proximal hydroureter and the IVU showed right renal hydronephrosis with delayed excretion and drainage (grade II) with s shape of the upper segment of the right ureter, and we considered IVU result as a diagnosis.
Surgery is required in symptomatic patients or in those with worsening kidney function. The standard repair of retrocaval ureter is open surgical pyelopyelostomy [3]. Repair usually involves open or laparoscopic resection of the redundant retrocaval ureteral segment, anteposition and ureteroureteral or ureteropelvic anastomosis [4]. Here we did an open surgery. After putting the patient in right flank position, the right ureter was separated first. We found the construction in level L2 and L3. We cut the constructed segment and anastomed both endings after inserting a double-j stent. Following up the patient by ultrasound is the most important part in the treatment.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}