





Abstract
The design of and applications for wrist arthroplasty continue to evolve but lag behind the results for hip and knee arthroplasty with respect to demonstrable durability and effectiveness. As we develop our knowledge, experience and the indications for wrist replacement surgery, it is important that we learn from past design and surgical experience. We report the case of a female patient treated with a Motec cementless metal-on-metal wrist replacement (Swemac Orthopaedics AB, Linköping, Sweden) for post-traumatic arthritis of the radiocarpal joint. Based on our experience with this case and others, we make two specific technical recommendations to improve the success and longevity of this implant.
INTRODUCTION
The design of and applications for wrist arthroplasty continue to evolve but lag behind the results for hip and knee arthroplasty with respect to demonstrable durability and effectiveness. As we develop our knowledge, experience and the indications for wrist replacement surgery, it is important that we learn from past design and surgical experience. The Motec total wrist replacement (Swemac Orthopaedics AB, Linköping, Sweden) is a modern implant which has been shown to be a good motion preserving alternative to wrist fusion [1]. We report the case of a female patient treated with a Motec cementless metal-on-metal wrist replacement for post traumatic arthritis of the radiocarpal joint.
CASE REPORT
A 52-year-old female patient presented following failed fixation of a left distal radius fracture. She had undergone surgical fixation of a distal radius fracture 8 years previously and now complained of persistent and continuous pain, restricted range of movement and functional limitation. Her imaging confirmed a healed distal radius fracture in neutral alignment but with evidence of degenerative change in the radiocarpal joint and migration of the metalwork so that the distal screws penetrated the wrist joint (Fig. 1A and B).

(A and B) PA and lateral radiographs showing failed distal radius fixation with radiocarpal degenerative change.
Following appropriate consultation and consent, she underwent total wrist arthroplasty. She reported complete pain relief and an improved range of movement. Ten weeks following surgery the patient presented in the emergency department following a fall. She landed heavily on the dorsiflexed hand and wrist, immediately noticing a change. Imaging confirmed that she had sustained a periprosthetic fracture in the middle finger metacarpal with dorsal displacement of the implant (Fig. 2A and B). Following a trial of non-operative treatment, she underwent revision surgery. The distal metacarpal implant was removed and replaced with a longer implant and the metacarpal fracture defect region was reinforced with autologous bone graft (Fig. 3A and B).

(A and B) PA and lateral radiographs showing a periprosthetic fracture around the metacarpal implant of a Motec wrist replacement.
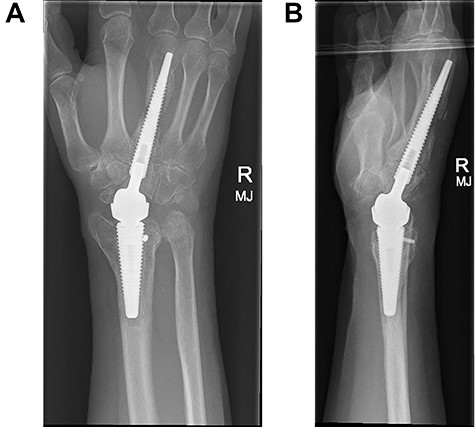
(A and B) PA and lateral radiographs following revision surgery to a longer metacarpal implant.
Three months following surgical treatment of her periprosthetic fracture, when reviewed in the outpatient clinic, the fracture had united and she demonstrated an excellent range of pain free motion and improved wrist function reflected in an improved PRWHE score from 66 preoperatively to 22, 3 months after surgery.
DISCUSSION
The Motec wrist replacement shares some design features with the earlier Biaxial wrist replacement (Depuy Orthopaedics Inc, Leeds, UK). Both are unconstrained implants with an intramedullary design sited in the middle finger metacarpal and the distal radius metaphysis. They are both usually implanted without cement fixation and rely on osseointegration which is encouraged with a porous coating on the implant. The Biaxial wrist replacement showed promising results but when failure occurred this was often as a result of loosening or dorsal migration of the distal metacarpal component. Takwale et al. showed that dorsal malalignment of the prosthesis was the strongest predictor for failure [2, 3]. This mechanism of failure was usually addressed with wrist arthrodesis as a salvage procedure. This did not appear to be a factor in this case however.
Distal implant loosening or malalignment did not appear to be factors in this case although we recognize that based on the similarities in design, these are important considerations. We propose two further technical points which we believe to be important for success with the Motec wrist replacement.
We recommend that the distal component should be positioned beyond the isthmus in the middle finger metacarpal to maximize the intramedullary fix, reduce any tendency to malalignment and any subsequent tendency towards dorsal migration of the implant. We would suggest that this is critical for success. We have found that it is easier and more likely that a short metacarpal implant will be implanted in unacceptable dorsal malalignment.
In this case, revision surgery with a longer metacarpal implant avoided the need for wrist fusion as a salvage procedure and it is now our routine practice to site the distal implant beyond the isthmus.
Fusion of the middle finger carpometacarpal joint reduces the bending moment around the metacarpal component of the implant and reduces the tendency of the distal implant to migrate dorsally. In this case, at revision surgery, this joint had not successfully fused and we recommend that attention to this step will also reduce the chance of failure.
We believe that attention to these technical points, relevant for previous wrist arthroplasty designs, will increase the success and reduce the risk of failure associated with the modern Motec wrist replacement.
STATEMENT OF INFORMED CONSENT
The patient described in this case report was informed that this case would be submitted for publication and has given their consent.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}