





Abstract
Abdominal complications after placement of ventriculoperitoneal (VP) shunt are commonly reported but asymptomatic bowel perforation with enterocutaneous fistula (ECF) is rare. This case describes a young male patient who underwent VP shunt for hydrocephalus 10 years ago. He presented with ECF due to the non-functioning abdominal end of the shunt. Patient was managed with laparotomy with fistulectomy with bowel resection and anastomosis. ECF is a rare complication of VP shunt.
INTRODUCTION
Ventriculoperitoneal (VP) shunt is a common neurosurgical procedure for drainage of cerebrospinal fluid (CSF) into the peritoneal cavity [1]. Abdominal complications such as abdominal wall perforation, ascites, CSF fluid fistula, hernia, hydrocele, scrotal extrusion, ileus, intramuscular cysts, intussusception, migration of the peritoneal catheter, torsion, peritonitis, pseudocyst/tumor, vaginal and viscus perforation, and volvulus can occur in 10–30% of cases, and bowel perforation can occur in 0.1–1.0% of cases [2–4].
Few cases of enterocutaneous fistula (ECF) due to VP shunt have been reported in literature. Possible mechanisms for intra-abdominal complications include chronic low-grade inflammatory reaction and fibrous encapsulation secondary to irritation from catheter, infected CSF or sterile xanthochromic CSF [2]. Fibrosis has an anchoring effect on tube causing ulceration of bowel wall and perforation [4]. Perforation peritonitis is seen in <15–25% of cases [5–7]. Therefore, the diagnosis of ECF due to VP shunt is difficult.
CASE REPORT
A 33-year-old male presented to the outpatient department with complaints of repeated discharge from root of penis on right side for 2 years. The condition was initially diagnosed as subcutaneous abscess with and treated with incision and drainage. The patient underwent incision and drainage two times. The discharge persisted even after repeat incision and drainage. Sinogram using water soluble contrast was planned to identify the cavity and its extension. Sinogram showed opacification of abdominal end of ventriculostomy tube superiorly with contrast spilling out from the distal ileum and opacification of the cecum, ascending colon and distal ileum. The findings were consistent with asymptomatic distal ileal perforation by ventriculostomy tube with sinus wound at the root of the penis on right side (Fig. 1).
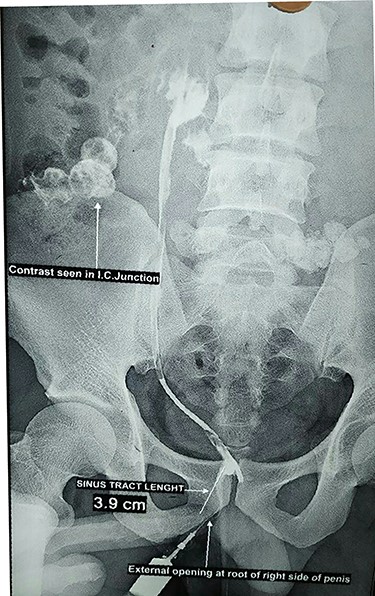
Sinogram
The patient was referred for neurosurgery consultation. Computed tomography (CT) of head was done which showed the proximal end in basal cistern. The ventricles were not dilated. Laparotomy was planned along with VP shunt revision. At laparotomy, the abdominal end of shunt was found traversing the terminal ileum ~12 cm proximal to ileocecal junction (Figs 2–4). Fistulectomy with ileal resection and anastomosis was done. The abdominal end of VP shunt was fractured with no connection to the proximal end. The fractured abdominal end of the shunt was removed. The proximal end was tied as it was not functioning. Fistula tract at the root of penis was excised through a separate incision.
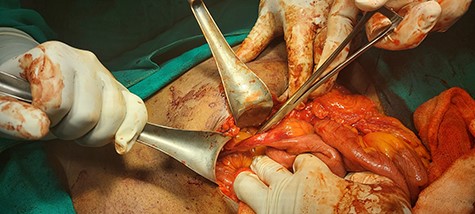
Proximal end of shunt traversing through ileum
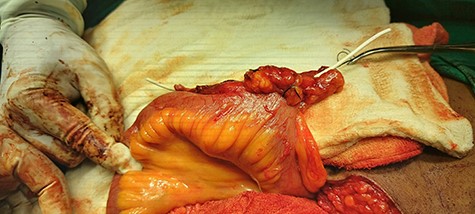
Shunt tract
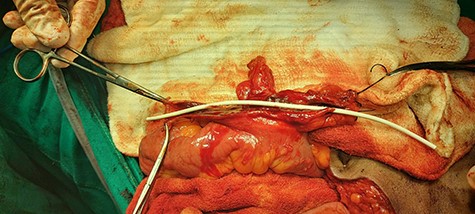
Fistula tract opened
The postoperative period was uneventful. Patient was discharged on 10th postoperative day and is doing well on follow-up.
DISCUSSION
Peritoneal complications are common with VP shunt [1–4]. The complications can present with acute onset or can be asymptomatic for a long time as in our case. The reason our patient did not present with ventricular infection could be because of the detachment of abdominal end with cranial end of the shunt.
The exact mechanism for the fistulisation could not be explained in our patient, but various mechanisms such as chronic low-grade inflammatory reaction and fibrous encapsulation secondary to irritation from catheter, infected CSF or sterile xanthochromic CSF have been speculated [2–4]. Sells and Loeser [5] and Yousfi et al. [6] have reported clinical peritonitis in <15–25% of cases. Voronovich et al. reported a 2-year-old boy with post-infectious hydrocephalus, managed with a VP shunt and complicated by shunt extrusion through the cranial skin. The shunt was removed due to concern for infection, and the child was found to have an ECF communicating along the shunt track between the small bowel and a clavicular sinus [8]. Rinker et al. reported a case of an abandoned abdominal VP shunt that migrated into the gastric antrum, colonic hepatic flexure and liver parenchyma, which was discovered incidentally on an abdominal CT, obtained for renal stones [9].
In conclusion, asymptomatic bowel perforation with ECF is a rare complication of VP shunt.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
CARE GUIDELINES
The manuscript was prepared based on the CARE guidelines.
CONSENT FOR PUBLICATION
Written informed consent was taken from the patient and patient party for publication of this report.
COMPETING INTERESTS
The authors have no competing interest for the publication of this case report.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
All costs incurred during the collection of data and preparation of this manuscript have been covered by the authors.
AUTHORS’ CONTRIBUTIONS
P.J. and B.D.J. carried out the conception and design of the study. P.J. and B.D.J. acquired the data. P.J. and B.D.J. analyzed and interpreted the data. B.D.J. critically revised the manuscript and gave the final approval. All authors read and approved the final manuscript.
ACKNOWLEDGEMENT
The authors would like to thank the patient and patient party who stood tough and gave permission for the publication of this case report.

{kind=link}
{kind=link}
{kind=link}
{kind=link}