





Abstract
Subtalar dislocations are rare injuries that typically occur from high-energy injuries. All subtalar dislocations should be attempted to be closed reduced, however, ~32% are irreducible requiring open reduction. We present an irreducible medial subtalar dislocation following a motor vehicle accident with no associated fractures demonstrated on radiograph. However, open reduction revealed an incarcerated anterior talar head fracture that was reduced and stabilized with retrograde K-wires.
INTRODUCTION
A subtalar dislocation is a rare injury which accounts for only 1–2% of all adult joint dislocations [1]. These dislocations usually result from high-energy injuries due to the strong ligamentous connections in the ankle [2]. Common mechanisms include motor vehicle accidents, falls from height and occasionally sports. A subtalar dislocation involves disruption of both the talocalcaneal and talonavicular joints which can displace the midfoot medially, laterally, anteriorly or posteriorly. About 80% of all subtalar dislocations occur medially, while 15–20% occur laterally [3]. Anterior and posterior subtalar dislocations are extremely rare, but both have been reported [4, 5].
Subtalar dislocations commonly have other associated injuries in the ankle. The tibia, fibula, calcaneus and navicular are the most commonly fractured bones, but the cuboid, cuneiforms and metatarsals are at risk as well [6]. In fact, one study demonstrated that ~88% of all patients with a subtalar dislocation had an associated foot or ankle injury [2]. First line treatment for these dislocations is closed reduction under sedation. However, 32% of dislocations can be irreducible even with adequate sedation, especially with higher energy mechanisms of injury [2].
In this case study, we report a medially displaced subtalar dislocation that was unable to be successfully closed reduced and retrospectively thought to be caused by an incarcerated anterior talar head fracture fragment not apparent on radiographs.
CASE REPORT
This patient is a 30-year-old male who presented to our emergency room following a head-on motor vehicle accident as a restrained driver. He described pain in his right ankle immediately after the accident and was taken to the emergency department as a trauma alert. ATLS protocol was instituted but no other injuries were identified. The patient’s right ankle was grossly deformed and locked in supination but skin was intact (Fig. 1). The right lower extremity was neurovascularly intact. Initial X-rays (Fig. 2) of the right ankle demonstrated a medial subtalar dislocation without associated fractures. In the emergency department, closed reduction was attempted under conscious sedation but was unsuccessful. Therefore, risks, benefits and alternatives were discussed and the patient elected to proceed with urgent closed vs open reduction of the right subtalar joint and any other indicated procedures.

Patient’s right ankle.

Presenting X-rays of the right ankle.
Once general anesthesia was induced, closed reduction was attempted using axial traction with the knee in flexion. Closed reduction was unsuccessful once again (Fig. 3) so the decision was made to attempt open reduction. An anteromedial approach was used dissect down to the talonavicular joint. Retractors were placed with care to avoid injury to tibialis anterior tendon or superficial peroneal nerve. The joint capsule was seen to be disrupted and further exposure revealed a thin, coronal fracture of the anteromedial aspect of the talar head measuring roughly 2 cm in length and 6 mm in thickness (Fig. 4). Once this fragment was removed, the subtalar and talonavicular joints were easily reduced. It was thought that this incarcerated fragment was the likely cause for the unsuccessful closed reduction. The talar head fragment was unamendable for stabilization due to its small size with poor healing potential, thus it was removed. The talonavicular joint was then percutaneously pinned in retrograde fashion with three K-wires (Fig. 5) to maintain anatomic reduction of the subtalar and talonavicular joints and the foot was splinted. At 2 weeks follow-up the patient was doing well and radiographs revealed no interval loss of reduction (Fig. 6).

Intraoperative AP view localizing the medial subtalar dislocation.
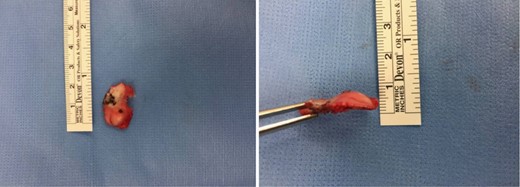
Anteromedial talar head fragment.

Intraoperative fluoroscopy status-postreduction and fixation.
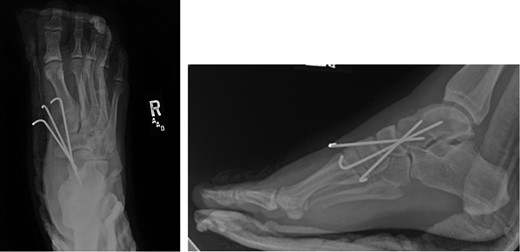
Two-week postoperative plain films.
DISCUSSION
In our case report, we describe a medial subtalar dislocation which was irreducible by closed technique due to an anteromedial talar head fracture fragment blocking the reduction. Other anatomical structures reported to block the reduction of medial subtalar dislocations include the talonavicular joint capsule, extensor digitorum brevis (EDB), buttonholing of the talar head through the EBD, dorsalis pedis arterial branches or even the deep peroneal nerve [7]. In this case, it was clear upon surgical exposure that no structures other than the talar head fragment were interposed.
As previously mentioned, the talar head fragment found intraoperatively was not identified on radiographs. One article suggests obtaining a CT scan of the ankle to assess for fractures [8]. In this case, the patient was taken to the OR urgently due to his irreducible dislocation and thus a CT scan would not change management.
Some studies suggest obtaining a CT scan of the ankle postreduction to check anatomic reduction as well as assess for other fractures [8, 9]. In our case, we did not obtain a postreduction CT scan. The subtalar and talonavicular joint were well visualized intraoperatively and were found to have no other associated fractures. In addition, anatomic reduction was obtained and under direct visualization and confirmed with fluoroscopy. Due to residual instability following reduction, K-wires were used to stabilize and hold the reduction. K-wire transfixation is supported in the literature for subtalar dislocations which tend to redislocate [10]. In other cases, where the joint is stable after reduction, there is no need for fixation.
It is currently too early to assess our patient postoperatively; however, it is imperative that patients begin physical therapy as soon as possible to limit the degree of joint stiffness and arthritis in the subtalar joint.
CONCLUSION
In the case report presented, a medially displaced subtalar dislocation was found to be irreducible using closed techniques. During open reduction, an anteromedial talar head fracture fragment was found be blocking the reduction. Once removed, the dislocation was easily reduced, but still unstable. Three K-wires retrograde percutaneous K-wires were placed across the talonavicular joint to hold the reduction. Short-term follow-up has been unremarkable.
ACKNOWLEDGEMENTS
None.
CONFLICT OF INTEREST STATEMENT
None

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}