





Abstract
A 43-year-old female noticed hematochezia and lower-right abdominal pain during menstruation. Her family doctor detected a mass by computed tomography at the ileocecum. She was referred to our hospital and colonoscopy was performed. We observed extrinsic pressure resulting in mucosal change at the ileocecum. We also observed a submucosal tumor-like lesion at the rectosigmoid. We performed biopsy from both lesions, both were benign. Ileocecal resection and rectal low anterior resection were performed for diagnosis. Redness, induration and serosal dimpling were recognized at the ileocecum, rectosigmoid and upper rectum. All lesions had endometorial tissue in muscular layer, so pathological diagnosis was bowel endometriosis. Bowel endometriosis occurring in multiple parts and where two colectomies were performed simultaneously is very rare. To determine the optimal method of treatment for the bowel endometriosis, detailed preoperative examination must be performed, specifically complete surgical resection of the lesion for definite diagnosis.
INTRODUCTION
Endometriosis is a disease where endometrial tissue presents outside of the endometrium or myometrium [1]. It occurs in ~6–10% of the females of reproductive age [1].
We experienced a case of bowel endometriosis treated with simultaneous ileocecal and rectal resection. There were three reasons to perform simultaneous resection: lesions occurred in the two different parts, definite diagnosis was not made, or bowel stenosis was detected. Bowel endometriosis occurring in the multiple parts and where two colectomies were performed simultaneously is very rare.
CASE PRESENTATION
A 30-year-old woman underwent left ovariectomy and right ovarian endometrioma resection. At 40 years old, she noticed hematochezia and right-lower abdominal pain during menstruation, the symptoms continued over 3 years. At 43 years old, although she no longer noticed the same symptoms, she had right-side chest and back pain during menstruation so visited the doctor. A tumor of the ileocecum and right pneumothorax were discovered by computed tomography (CT). Pneumothorax was improved by conservative treatment. Submucosal tumor (SMT) was discovered at the rectosigmoid (RS) by colonoscopy (CS). The patient was referred to our hospital. A 3 cm size mass was discovered in the right-lower abdomen. Rectal examination was unremarkable and laboratory data was normal. CS showed the SMT with erosion at RS (Fig. 1a). As the scope could not pass through the sigmoid colon, we used the double balloon endoscopy. We observed erythrogenic mucosa of the ileum resembling salmon roe (Fig. 1b), and the cecum was suppressed from the outside. Biopsy was taken from the RS and ileum, but the pathological result was benign. Endoscopic ultrasound guided fine needle aspiration was also performed from the RS, but no abnormal cell were observed. By abdominal CT, a mass lesion was recognized at the ileocecum. No abnormal lesions were recognized at the rectum (Fig. 2).
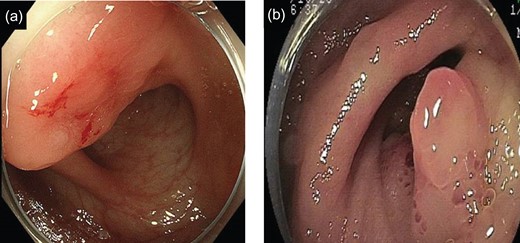
(a) Endoscopic findings of RS: A SMT-like lesion was observed. (b) Endoscopic findings of ileocecum: A salmon roe-like formation of erythrogenic mucosa at the ileum end was observed.

CT revealed a mass of ileocecum (arrow).
Preoperative diagnosis was tumor of the ileocecum and SMT of the rectum. The patient has a history of hematochezia and abdominal pain during menstruation, and received resection of the endometrioma. Thus, endometriosis was considered as differential diagnosis. Definitive diagnosis could not be confirmed, however, surgery was performed because the symptoms were so severe.
Operative findings: On lower-midline incision, induration with red serosal dimpling was observed at the ileocecum. The same finding was observed at the RS and upper rectum. The uterus was enlarged and the right ovary was normal. First, ileocecal resection was performed, then lower-rectum anterior resection was performed.
Specimen: Strong dimpling of the serosa on rectum and ileocecum was recognized (Figs 3a, b and 4a, b).
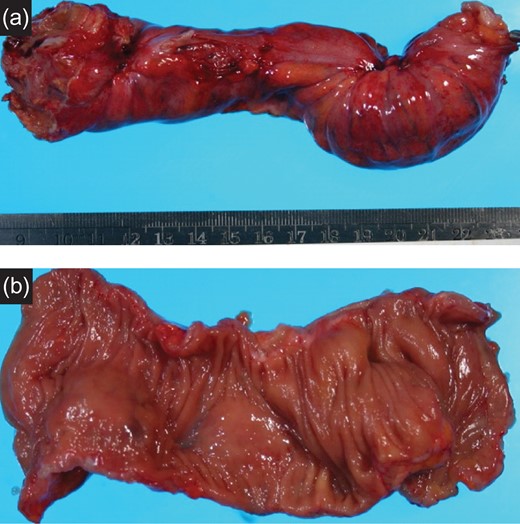
(a) Resected specimen (rectum): The serosal dimpling was observed. (b) Resected specimen (rectum): A SMT-like lesion was observed.
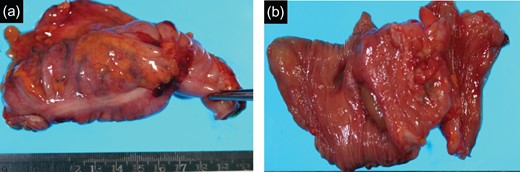
(a) Resected specimen (ileocecum): Serosal dimpling was also observed. (b) Resected specimen (ileocecum): A SMT-like lesion was also observed.
Pathological findings: Fibrosis and the ecchymosis were pathologically observed. Endometrial tissue was seen at the muscular layer indicated ecchymosis. There were no malignant cells or lymph node metastasis (Fig. 5a, b).
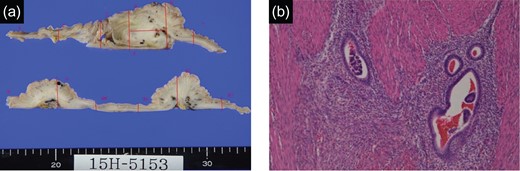
(a) Specimen (rectum): Contractures and ecchymosis were recognized. (b) Specimen (rectum, H.E. staining): Endometrial tissue was found in ecchymosis in muscularis.
Final diagnosis was endometriosis in the bowel, ileocecum and rectum. The postoperative course was good and the patient was discharged on ninth postoperative day. The patient is now on a course of corpus luteum hormone.
DISCUSSION
Endometriosis is a disease where the endmetorium expands beyond the uterus. As chronic inflammation occurs, dysmenorrhea, pelvic pain and infertility can develop [2]. Endometriosis is reported in 6–10% of women of reproductive age [1], with some reports as many as 15% [3]. Endometriosis is classified in three types: peritoneal endometriosis, endometriotic ovarian cysts and deeply infiltrative endometriosis (DE) [3]. This patient met DE group classification. By definition, DE is where lesions infiltrate beyond 5 mm from serosa into muscular layer within the peritoneum. About 10% of endometriosis occurs in the bowel, 80–90% of reported cases occur in rectum and sigmoid colon [1, 3]. Clinical symptoms are pelvic pain, infertility, menstrual pain, constipation, diarrhea, tenesmus and rectal bleeding [3]. Differential diagnosis includes inflammatory bowel disease, solitary rectal ulcer syndrome and rectal tumor [3]. For diagnosis of endometriosis, presented symptoms and physical findings are most important, but transvaginal ultrasonography, barium enema examination and magnetic resonance imaging (MRI) are also useful [1–3]. In this case, from the characteristic symptoms, endometriosis was suspected in differential diagnosis. Effective transvaginal ultrasonography depends on the physician’s skill and experience [2], but other meta-analysis reported that 91% sensitivity and 98% specificity [4]. Barium enema examination is also useful in predicting lesions range and depth [3, 4]. The usefulness of MRI jelly was also reported [5].
In summary, as other methods vary in usefulness, to correctly make diagnosis, it is necessary to retrieve tissue by surgical intervention, and laparoscopy is often performed [1–3]. Concerning therapy, it is important to remove pain, prevent recurrence and keep fertility. Surgery is said to be effective in resolving symptoms such as pain [2, 6]. It is very important to completely remove endometrial tissue by surgery [1–3]. Laparoscopy is reported to have fewer postoperative complications and superior fertility retention, but there are also reports stating no difference in improvement of pain and quality of life [7].
In the present case, the patient required operation for endometrioma, so laparotomy was performed to remove the lesion completely. There are several methods of lesion resection, such as discotic resection, intestinal partial resection and resection by CO2 laser [2, 3, 6, 8]. But, if the resection range extends to over half of the intestinal tract, total intestinal resection is necessary [3]. In this case, the lesion extended to over half of the tract and stenosis was doubted, so intestinal resection was performed on both the ileocecum and rectal lesion. The recurrence rate of endometriosis in patients receiving intestinal resection is reported between 4.7 and 25% with follow up over 2 years [6].
We encountered a very rare case of bowel endometriosis in both the ileocecum and the rectum at the same time. Our case was severe, so optimal treatment was surgery. However, this may not always be the case, depending on severity. It is necessary to consider the method of treatment for bowel endometriosis, such as drug treatment, surgery and whether bowel resection is required.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
The authors declare no financial or any other type of support.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}