





Abstract
Intestinal myxoma is among the rarest presentations of this benign tumour. Moreover, the association of an intestinal myxoma and a mesenteric lipoma is even more surprising. Intestinal tumours are often diagnosed inadvertently: a routine physical exam may identify these tumours or an abdominal computed tomography scan or abdominal ultrasound for another indication. Acute intestinal obstruction is rare. We hereby report the case of a 6-year-old boy who presented in the emergency room of our institution with acute intestinal obstruction and the management of this case.
CASE REPORT
We report the case of a 6-year-old boy who presented at the Emergency Room (ER) of our institution with severe abdominal pain and vomiting. History of presenting complain revealed that one week prior to the consultation, the patient started complaining of intense and progressive pain, initially epigastric but later peri-umbilical. The pain was paroxysmal, without any irradiation and no remitting or exacerbating factor. Three days after the onset of the pain, there was a complete stoppage of stool passage with vomitus which initially was food and later biliary. This prompted the personal administration of Albendazole by the mother but with the persistence of the clinical picture she rapidly brought the child the ER. The past-history was non-contributory. Upon arrival, the patient was anxious, and physical exam revealed a conserved general state, stable vitals, an obstructive syndrome, an irregular umbilical mass, with no abdominal distention and no signs of dehydration. A plain abdominal radiograph revealed an agglutination of distended colonic segments in the left upper quadrant (Fig. 1). An abdominal ultrasound was also conducted and showed a cystic abdominal mass. Complete blood count revealed moderate anaemia. Horizontal laparotomy was done and found a twisted small bowel obstruction with a large encapsulated yellowish mass inserted with a small base on the anti-mesenteric aspect of the ileum measuring 10×15 cm2 at 30 cm away from the ileo-colic junction without any adhesions. On the same insertion but rather on the mesenteric aspect was a smaller greenish mass (3 × 5 cm2) giving a granulated feeling on palpation. There also were numerous lymph nodes on the mesentery. Small bowel bulk resection of 10 cm was done and intestinal end-to-end anastomosis also. Histopathology confirmed the mesentery lipoma and the associated structure to be a myxoma. Post-operative progress notes return of peristalsis and stool from Day 3 post-op (Fig. 2).

Small bowel strangulation and lipoma.
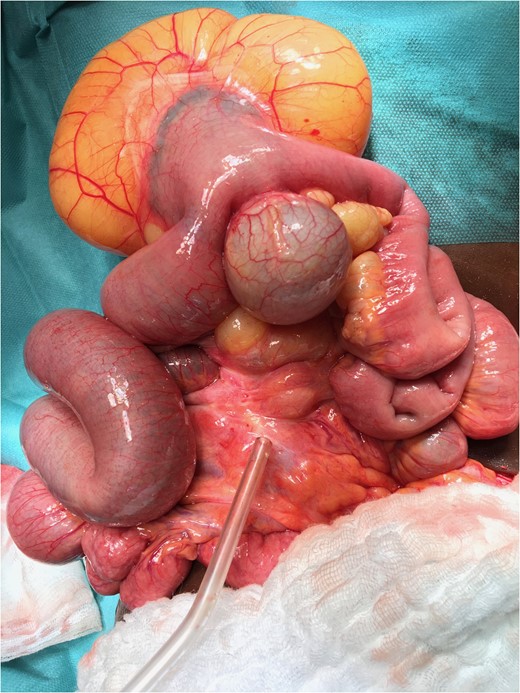
Lipoma and myxoma.
DISCUSSION
Lipomas are common benign tumours developing from mature fat cells. They often are found on the superficial aspects of the body and rarely are they deep-seated [1, 2]. No aetiology for lipomas has been identified but an association with diabetes, raised cholesterol, obesity has been proven [3]. Amongst all the deep locations of lipomas in childhood, the mesenteric location is the rarest (Fig. 1) [4]. The latter is often found in adulthood between 40 and 60 years. Apart from a lipoma, our patient had a myxoma which is extremely rare in this location. They are more common in the heart and originate from mesenchymal tissue. They are benign and when found in the gastrointestinal tract, yields intussusception [5]. Stout [6] reported a series of five cases of intestinal myxomas and of these, himself saw one. The particularity of this case is that it occurs in childhood and does not present with intussusception as described by authors like Varsamis et al., who report this finding to be more common in middle-aged women and present with intussusception [5–7]
Lipomas rarely call for concern since they often are superficially located and only give rise to aesthetic worries from patients. When lipomas are located intra-abdominally, the symptoms more often are vague and often misleading. The diagnosis of mesenteric lipomas is usually incidental but children may present with abdominal pain, vomiting, abdominal distention and rarely with intestinal obstruction as was observed in our case who presented with intestinal obstruction syndrome. When the tumour is located closest to the intestinal lumen, due to compression, it gives rise to obstructive symptoms but allows peristalsis progression of the bowel [8]; this is different from what we observed with a complete volvulus and progressively increasing pain (Fig. 2).

Plain abdominal radiograph.
The gold standard imaging modality for mesenteric lipomas could be computed tomography scans and or magnetic resonance imaging but as a result of the limited availability of such an equipment in our setting, ultrasonography was used [3]. Mesenteric lipoma ultrasonography shows a homogenous well-encapsulated mass which echogenic (Fig. 3) [9].
Since mesenteric lipomas have a low recurrence rate and small malignant potential, complete surgical resection could be a suggested treatment modality for this group of patients. In our case, we observed regression of symptoms after surgery.
CONCLUSION
Reporting this case should raise awareness on the fact that there could be an association of two rare intestinal tumours in children and abdominal differential diagnoses for intestinal tumours should include these tumours which are rare but may present in even more misleading signs and symptoms.
ACKNOWLEDGEMENTS
Regards to the patient and family for giving consent.
CONFLICT OF INTEREST STATEMENT
Authors report no conflict of interest.

{kind=link}
{kind=link}
{kind=link}